
Gefitinib, tablet, 250 mg, Iressa® - November 2012
PDF printable version of this page (PDF 91KB)
Public Summary Document
Product: Gefitinib, tablet, 250 mg, Iressa®
Sponsor: AstraZeneca Pty Limited
Date of PBAC Consideration: November 2012
1. Purpose of Application
The submission sought Medicare Benefits Schedule (MBS) listing of epidermal growth factor receptor (EGFR) mutation testing and to extend the current Authority Required Pharmaceutical Benefits Scheme (PBS) listing to include first line treatment of locally advanced or metastatic non-small cell lung cancer (NSCLC).
2. Background
Gefitinib is currently PBS listed for the treatment, as monotherapy, of locally advanced or metastatic non-small cell lung cancer in patients with a WHO performance status of 2 or less, where disease progression has occurred following treatment with at least one chemotherapy agent and there is evidence that the patient has an activating mutation(s) of the EGFR gene in tumour material.
Gefitinib was recommended for listing at the July 2004 meeting of the PBAC on the basis of acceptable cost-effectiveness compared with docetaxel and best supportive care for patients with an activating mutation of the EGFR gene. Listing was effective from 1 December 2004.
At the March 2008 meeting, the PBAC considered a sponsor request to amend the PBS restriction by removal of the requirement for the activating EGFR mutation and alignment with the TGA indication at that time, which specified two patient subgroups eligible for gefitinib: those who have never smoked and those taking gefitinib who have demonstrated some benefit. The PBAC considered that inadequate evidence was provided to allow an assessment to be made on the cost-effectiveness of gefitinib in the population that would be covered under the requested listing and that more detailed information from a recent clinical trial was required. PBAC therefore recommended no changes be made to the PBS listing for gefitinib pending a further submission from the sponsor.
At its November 2009 meeting, the PBAC recommended an amendment to the current PBS restriction by removing the requirement that analysis of the DNA sequence of the EGFR gene must be used to detect a mutation in the EGFR gene. The PBAC noted that the analysis by DNA sequencing methodology was not MBS reimbursed and it was therefore considered reasonable to use other methodologies to detect the specific activating mutations in the EGFR gene.
At the November 2010 meeting, the PBAC rejected a submission seeking a first-line listing for gefitinib for the treatment of patients with locally advanced or metastatic non-small cell lung cancer (Stage IIb/IV NSCLC) who have an activating mutation in the epidermal growth factor receptor gene (EGFR M+), on the basis of unacceptably high and uncertain cost-effectiveness. The main uncertainties related to the prevalence of EGFR M+ in unselected Australian NSCLC patients, EGFR testing performance and cost, the effect of these on the comparative treatment effect of first-line gefitinib, and the extent of the incremental QALY gain based on quality of life advantages without any overall survival advantage.
3. Registration Status
Gefitinib has been TGA registered since 28 April 2003. The TGA registration for gefitinib was revised on 12 July 2010. It is currently indicated for the treatment of patients with locally advanced or metastatic NSCLC, whose tumours express activating mutations of the EGFR tyrosine kinase.
4. Listing Requested and PBAC’s View
Authority Required
Initial PBS-subsidised treatment, as monotherapy, of locally advanced or metastatic
non-small cell lung cancer in patients with a WHO performance status of 2 or less,
where:
(1) disease progression has occurred following treatment with at least 1 chemotherapy
agent; and
(2) there is evidence that the patient has an activating mutation(s) of the epidermal
growth factor receptor (EGFR) gene in tumour material.
Authority Required
Continuing PBS-subsidised treatment, as monotherapy, of locally advanced or metastatic
non-small cell lung cancer in patients with a WHO performance status of 2 or less,
where the patient has previously been issued with an authority prescription for gefitinib.
Authority Required
Initial PBS-subsidised treatment, as monotherapy, of locally advanced or metastatic
(Stage IIIB/IV) non-small cell lung cancer (NSCLC) in patients with:
(1) a WHO performance status of 2 or less, and;
(2) a diagnosis of non-squamous NSCLC, and;
(3) evidence that tumour material is expressing exon 19 deletions or exon 21 point
mutation L858R of the epidermal growth factor receptor (EGFR) gene; OR
there is evidence that the patient has an activating mutation(s) of the epidermal
growth factor receptor (EGFR) gene in tumour material.
Authority Required
Continuing PBS-subsidised treatment in patients where the patient has previously been
issued with an authority prescription for gefitinib.
Note:
Tyrosine kinase inhibitors should not be used in people with confirmed EGFR mutation
negative NSCLC.
For PBAC’s view, see Recommendation and Reasons.
5. Clinical Place for the Proposed Therapy
The submission proposed that gefitinib is an alternative to chemotherapy in the treatment of patients with EGFR M+ NSCLC.
6. Comparator
The resubmission nominated carboplatin and paclitaxel as the main comparator. This combination was used in two of the gefitinib clinical trials (IPASS and NEJ002).
For PBAC’s view, see Recommendation and Reasons.
7. Clinical Trials
The submission presented the IPASS and First-SIGNAL trials to provide evidence of the effectiveness of gefitinib compared to platinum-based doublet chemotherapy (carboplatin plus paclitaxel and cisplatin plus gemcitabine, respectively) in patients with locally advanced or metastatic NSCLC of the adenocarcinoma subtype. The IPASS and First-SIGNAL trials were included in the November 2010 submission and were presented in the resubmission with updated overall survival (OS) data. Updated progression free survival (PFS) data were provided for the First-SIGNAL trial.
The resubmission included two other trials presented in the 2010 submission, the NEJ002 (Maemondo et al) and WJTOG3405 (Mitsudomi et al) trials, which investigated the effectiveness of gefitinib compared to platinum-based doublet chemotherapy in the first-line treatment of patients with advanced or metastatic NSCLC who had an EGFR mutation. The NEJ002 and WJTOG3405 trials were conducted with a population of treatment naive stage IIIB or IV NSCLC patients who had EGFR gene mutations.
The approach taken in the resubmission was to present retrospective evidence of the effect of gefitinib on EGFR M+ and M- NSCLC compared with platinum-based doublet chemotherapy (IPASS and First-SIGNAL trials),and to supplement this with evidence concerning the effectiveness of gefitinib in treating EGFR M+ NSCLC (NEJ002 and WJTOG3405 trials), the prevalence of EGFR mutations among patients with non-squamous NSCLC and the diagnostic performance of EGFR mutation testing methods.
The table below details the published trials presented in the submission.
|
Trial ID/First Author |
Protocol title/ Publication title |
Publication citation |
|---|---|---|
|
Direct evidence - randomised trial(s) |
||
|
Iressa Pan Asia Study (IPASS) |
||
|
Mok TS et al. |
Gefitinib or Carboplatin-Paclitaxel in Pulmonary Adenocarcinoma. Clinical Outcomes of Patients with Epidermal Growth Factor Receptor (EGFR) Mutations in IPASS (IRESSA Pan Asia Study). |
New England Journal of Medicine (2009); 361 (10): 947-57 13th World Conference on Lung Cancer, San Francisco 31 July, 2009 |
|
Ohe Y et al. |
Phase III, randomized, open-label, first-line study of gefitinib versus carboplatin/paclitaxel in selected patients with advanced NSCLC (IPASS): Evaluation of recruits in Japan. |
Journal of Clinical Oncology (2009); 27 (15): 8044 |
|
Fukuoka M et al. |
Biomarker analyses from a phase III, randomized, open-label, first-line study of gefitinib versus carboplatin/ paclitaxel in clinically selected patients with advanced NSCLC in Asia (IPASS). |
Journal of Clinical Oncology (2011); 29 (21): 2866-2874 |
|
Yang CH et al. |
Final overall survival results from a phase III, randomised, open-label, first-line study of gefitinib v carboplatin/ paclitaxel in clinically selected patients with advanced NSCLC in Asia (IPASS). |
Annals of Oncology (2010); 21: viii1-viii2 |
|
Thongprasert S et al. |
Health-related quality-of-life in a randomized phase III first-line study of gefitinib versus carboplatin/paclitaxel in clinically selected patients from Asia with advanced NSCLC (IPASS). |
Journal of Thoracic Oncology (2011); 6 (11): 1872-1880 |
|
Thongprasert S et al. |
Quality of life in a randomized phase iii first-line study of gefitinib vs carboplatin/paclitaxel in clinically selected Asian patients with advanced NSCLC (IPASS). |
European Lung Cancer Conference 2010, Abstract 205O, pp S80. |
|
Wu Y et al. |
Phase III, randomized, open-label, first-line study in Asia of gefitinib versus carboplatin/paclitaxel in clinically selected patients with advanced non-small-cell lung cancer: Evaluation of patients recruited from mainland China. Asia-Pacific |
Journal of Clinical Oncology (2012); In press |
|
Wu Y et al. |
Evaluation of clinically selected patients with advanced NSCLC recruited in China in a phase III, randomized, open-label, first-line study in Asia of gefitinib versus carboplatin/paclitaxel (IPASS). |
Journal of Clinical Oncology (2009); 27 (15): 8041 |
|
Wu Y et al. |
Tumour response, skin rash and health-related quality of life (HRQOL) - Post-HOC data from the IPASS study. |
European Journal of Cancer (2011); 47 (Suppl 1): S633-S634. |
| Yang J et al. |
Efficacy outcomes in first-line treatment of advanced NSCLC with gefitinib (G) vs carboplatin/paclitaxel (C/P) by epidermal growth factor receptor (EGFR) gene-copy number score and by most common EGFR mutation subtypes - Exploratory data from IPASS.
|
European Journal of Cancer (2011); 47 (Suppl. 1):S633. |
| First-SIGNAL | ||
| Lee YJ et al. |
Circulating cell-free DNA in plasma of never smokers with advanced lung adenocarcinoma receiving gefitinib or standard chemotherapy as first-line therapy. |
Clinical Cancer Research (2011); 17 (15): 5179-5187. |
| Han JY et al. |
First-SIGNAL: First-Line Single-Agent Iressa Versus Gemcitabine and Cisplatin Trial in Never Smokers With Adenocarcinoma of the Lung. |
Journal of Clinical Oncology (2012); 30 (10):1122-28. |
|
Lee JS et al. |
A Randomized Phase III Study of Gefitinib (IRESSA) versus Standard Chemotherapy (Gemcitabine plus Cisplatin) as a First-line Treatment for Never-smokers with Advanced or Metastatic Adenocarcinoma of the Lung. |
Journal of Thoracic Oncology (2009); 4(9), Supp 1. |
|
Linked evidence – diagnostic or predictive accuracy studies |
||
|
Endo K et al. |
Epidermal growth factor receptor gene mutation in non-small cell lung cancer using highly sensitive and fast TaqMan PCR assay. |
Lung Cancer |
|
Yatabe Y et al. |
A rapid, sensitive assay to detect EGFR mutation in small biopsy specimens from lung cancer. |
Journal of Molecular Diagnostics (2006); 8(3): 335-41. |
|
Ohnishi H et al. |
A simple and sensitive method for detecting major mutations within the tyrosine kinase domain of the epidermal growth factor receptor gene in non-small-cell lung carcinoma. |
Diagnostic Molecular Pathology (2006); 15(2): 101-8. |
|
Asano H et al. |
Detection of EGFR gene mutation in lung cancer by Mutant-Enriched Polymerase Chain Reaction Assay |
Clinical Cancer Research (2006); 12: 43-48. |
|
Takano T et al. |
Epidermal growth factor receptor mutation detection using high-resolution melting analysis predicts outcomes in patients with advanced non small cell lung cancer treated with gefitinib. |
Clinical Cancer Research |
|
Do H et al. |
High resolution melting analysis for rapid and sensitive EGFR and KRAS mutation detection in formalin fixed paraffin embedded biopsies. |
BMC Cancer (2008); 8: 142. |
|
Otani H et al. |
Detection of EGFR gene mutations using the wash fluid of CTguided biopsy needle in NSCLC patients. |
Journal of Thoracic Oncology (2008); 3(5): 472-6. |
|
Ellison G et al. |
A comparison of ARMS and DNA sequencing for mutation analysis in clinical biopsy samples |
Journal of Experimental & Clinical Cancer Research (2010); 29:132. |
|
Zhao J et al. |
A novel method for detection of mutation in epidermal growth factor receptor. |
Lung Cancer (2011); Mar 23. [Epub ahead of print] |
|
Borràs E et al. |
Clinical pharmacogenomic testing of KRAS, BRAF and EGFR mutations by high resolution melting analysis and ultra-deep pyrosequencing. |
BMC Cancer (2011); 11: 406. |
|
Kamel-Reid S et al. |
EGFR tyrosine kinase mutation testing in the treatment of non-small-cell lung cancer. |
Current Oncology (2012); 19(2): e67-74 |
|
Han H-S et al. |
Detection of EGFR mutation status in lung adenocarcinoma specimens with different proportions of tumour cells using two methods of differential sensitivity. |
Journal of Thoracic Oncology (2012); 7: 355–364 |
|
Goto K et al. |
An evaluation study of EGFR mutation tests utilised for non-small-cell lung cancer in the diagnostic setting. |
Annals of Oncology (2012 Jul 9); [Epub ahead of print] |
| NEJ002 |
No Clinical Study Report available. |
|
| Maemondo M et al. |
Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. |
New England Journal of Medicine (2010); 362 (25): 2380-2388. |
| Kobayashi Ket al. |
First-line gefitinib versus first-line chemotherapy by carboplatin plus paclitaxel
in NSCLC patients with EGFR mutations: A phase III study (002) by North East Japan
Gefitinib Study Group. |
Journal of Clinical Oncology (2009); 27(15): 8016 |
| Inoue A et al. |
Final overall survival results of NEJ002, a phase 3 trial comparing gefitinib to carboplatin plus paclitaxel as the first-line treatment for advanced NSCLC with EGFR mutations. |
Journal of Clinical Oncology (2011); 29 (suppl):abstract 7519 Abstract 9LBA at ECCO-ESMO |
| Inoue A et al. |
A randomized phase III study comparing gefitinib with carboplatin plus paclitaxel for the first-line treatment of NSCLC with sensitive EGFR mutations: NEJ002 study. |
European Journal of Cancer Supplement (2009); 7(2-3): 6 |
| Kinoshita I et al. |
Phase III study of gefitinib versus chemotherapy by carboplatin plus paclitaxel as first-line therapy for NSCLC with EGFR mutations: North east Japan gefitinib study group trial 002 (NEJ002). |
Respirology (2009); 14: A127 |
| Oizumi S et al. |
Quality of life with gefitinib in patients with EGFR-mutated non-small cell lung cancer: quality of life analysis of North East Japan Study Group 002 trial. |
The Oncologist (2012); 17 (in press) |
|
Satoh H et al. |
Low-dose gefitinib treatment for patients with advanced non-small cell lung cancer harboring sensitive epidermal growth factor receptor mutations. |
Journal of Thoracic Oncology (2011); 6 (8):1413-7 |
| WJTOG 3405 | ||
| Mitsudomi T et al. |
Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. |
The Lancet Oncology (2010); 11(2):121-8 |
| Tsurutani J et al. |
A phase III, first-line trial of gefitinib versus cisplatin plus docetaxel for patients with advanced or recurrent non-small cell lung cancer (NSCLC) harboring activating mutation of the epidermal growthfactor receptor (EGFR) gene: a preliminary result. |
Abstract O-9002 at ECCO-ESMO |
|
Mitsudomi T et al. |
Updated overall survival results of WJTOG 3405, a randomized phase III trial comparing gefitinib with cisplatin plus docetaxel as the first-line treatment for patients with non-small cell lung cancer harbouring mutations of the epidermal growth factor receptor (EGFR). |
Poster Session, June 5, 2012 |
|
Linked evidence - Meta-analyses of randomised trials |
||
|
Bria E et al. |
Outcome of advanced NSCLC patients harbouring sensitizing EGFR mutations randomised to EGFR tyrosine kinase inhibitors or chemotherapy as first-line treatment: a meta-analysis. |
Annals of Oncology (2011); 22: 2277-2285.
|
|
Edwards SJ et al. |
Tolerability of first-line treatments of locally advanced or metastatic non-small-cell lung cancer (NSCLC): A systematic review and adjusted indirect comparison. |
Value in Health (2010); 13 (7): A250. |
|
Edwards SJ et al. |
Gefitinib compared with doublet chemotherapy for first-line treatment of non-small-cell lung cancer (NSCLC): A systematic review and adjusted indirect comparison. |
Value in Health (2010); 13 (7): A252-A253. |
|
Goffin J et al. |
First-line systemic chemotherapy in the treatment of advanced non-small cell lung cancer: A systematic review. |
Journal of Thoracic Oncology (2010); 5 (2): 260-274. |
|
Gridelli C et al. |
Gefitinib as first-line treatment for patients with advanced non-small-cell lung cancer with activating epidermal growth factor receptor mutation: Review of the evidence. |
Lung Cancer (2011); 71 (3): 249-257. |
|
Ku GY et al. |
Gefitinib vs. chemotherapy as first-line therapy in advanced non-small cell lung cancer: Meta-analysis of phase III trials. |
Lung Cancer (2011); 74 (3): 469-473. |
|
Paz-Ares L et al. |
Clinical outcomes in non-small-cell lung cancer patients with EGFR mutations: pooled analysis. |
Journal of Cellular and Molecular Medicine (2010); 14(1-2):51-69. |
|
Petrelli F et al. |
Efficacy of EGFR Tyrosine Kinase Inhibitors in Patients With EGFR-Mutated Non-Small Cell-Lung Cancer: A Meta-Analysis of 13 Randomised Trials. |
Clinical Lung Cancer (2012); 13 (2):107-114. |
|
Gao G et al. |
Epidermal growth factor receptor-tyrosine kinase inhibitor therapy is effective as first-line treatment of advanced non-small-cell lung cancer with mutated EGFR: A meta-analysis from six phase III randomized controlled trials. |
International Journal of Cancer (2012); in press. |
8. Results of Trials
Progression Free Survival (PFS) results from IPASS and First-SIGNAL trials for the intention-to-treat (ITT) population and the retrospectively EGFR mutation-stratified population treated with either gefitinib or platinum-based doublet chemotherapy are shown in the table below.
|
|
Gefitinib
|
Platinum-based doublet chemotherapy |
Absolute difference
|
Hazard ratio (95% CI) |
|
IPASS |
Carboplatin + paclitaxel |
|
|
|
|
ITT population |
Number events 453/609 (74.7%) Median: 5.7 months |
Number events 497/608 (81.7%) Median: 5.8 months |
-0.1 months |
HR = 0.74 (0.65, 0.85) p < 0.0001 |
|
EGFR M+ |
Number events 97/132 (73.5%) Median: 9.5 months |
Number events 111/129 (86.0%) Median: 6.3 months |
+3.2 months |
HR = 0.48 (0.36, 0.64) p < 0.0001 |
|
EGFR M- |
Number events 88/91 (96.7%) Median: 1.5 months |
Number events 70/85 (82.4%) Median: 5.5 months |
-4.0 months |
HR = 2.85 (2.05, 3.98) p < 0.0001 |
|
EGFR mutation status unknown |
Number events 268/386 (69.4%) Median: 6.6 months |
Number events 316/394 (80.2%) Median: 5.8 months |
+0.8 months |
HR = 0.68 (0.58, 0.81) p < 0.0001 |
|
EGFR exon 19 mutations |
Number events 46/66 (69.7%) Median: 9.7 months |
Number events 65/74 (87.8%) Median: 5.6 months |
+4.1 months |
HR = 0.38 (0.26, 0.56) p < 0.0001 |
|
EGFR exon 21 L858R mutation |
Number events 48/64 (75.0%) Median: 9.1 months |
Number events 40/47 (85.1%) Median: 6.8 months |
+2.3 months |
HR = 0.55 (0.35, 0.87) p < 0.0001 |
|
First-SIGNAL |
Cisplatin + Gemcitabine |
|
|
|
|
ITT population (updated) |
Number events 153/159 (96.2%) Median: 5.8 months 1-year PFS 16.7% 2-year PFS 3.2% |
Number events 142/150 (94.6%) Median: 6.4 months 1-year PFS 2.8% 2-year PFS 1.4% |
-0.6 months |
HR = 1.20 (0.94, 1.52) p = 0.138 |
|
EGFR M+ (updated) |
n = 26 Median: 8.0 months 1-year PFS 34.6% |
n = 16 Median: 6.3 months 1-year PFS 14.3% |
+1.7 months |
HR = 0.54 (0.27, 1.10) p = 0.086 |
|
EGFR M- (updated) |
n = 27 Median: 2.1 months 1-year PFS 7.4% |
n = 27 Median: 6.4 months 1-year PFS 7.4% |
-4.3 months |
HR = 1.42 (0.82, 2.47) p = 0.226 |
CI = confidence interval; HR = hazard ratio; n = total participants in group.
Overall Survival (OS) results from IPASS and First-SIGNAL trials for the ITT population and the retrospectively EGFR mutation-stratified population treated with either gefitinib or platinum-based doublet chemotherapy are shown in the table below.
|
|
Gefitinib
|
Platinum-based doublet chemotherapy |
Absolute difference
|
Hazard ratio (95% CI) |
|
IPASS |
|
Carboplatin + paclitaxel |
|
|
|
ITT population (updated) |
Number deceased 484/609 (79.5%) Median survival 18.8 months |
Number deceased 470/608 (77.3%) Median survival 17.4 months |
+1.4 months |
HR = 0.90 (0.79, 1.02) p > 0.05 |
|
EGFR M+ (updated) |
Number deceased 104/132 (79%) Median survival 21.6 months |
Number deceased 95/129 (74%) Median survival 21.9 months |
-0.3 months |
HR = 1.00 (0.76, 1.33) p = 0.990 |
|
EGFR M- (updated) |
Number deceased 82/91 (90%) Median survival 11.2 months |
Number deceased 74/85 (87%) Median survival 12.7 months |
-1.5 months |
HR = 1.18 (0.86, 1.63) p = 0.309 |
|
First-SIGNAL |
|
Cisplatin + Gemcitabine |
|
|
|
ITT population (updated) |
Number deceased 113/159 (71.1%) Median: 22.3 months 1-year OS 74.2% 2-year OS 47.7% |
Number deceased 109/150 (72.7%) Median: 22.9 months 1-year OS 76.2% 2-year OS 47.4% |
-0.6 months |
HR = 0.93 (0.72, 1.21) p = 0.604 |
|
EGFR M+ (updated) |
n = 26 Median 27.2 months |
n = 16 Median 25.6 months |
+1.6 months |
HR = 1.04 (0.50, 2.18) |
|
EGFR M- (updated) |
n = 27 Median 18.4 months |
n = 27 Median 21.9 months |
-3.5 months |
HR = 1.00 (0.52, 1.91) |
|
EGFR mutation status unknown |
|
|
|
HR = 0.88 (0.64, 1.21) |
CI = confidence interval; HR = hazard ratio; n = total participants in group.
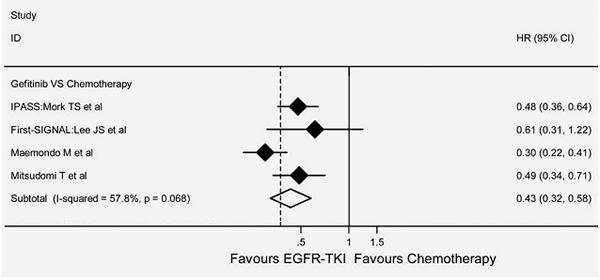
The PFS outcomes for the NEJ002 and WJTOG3405 trials were reported in the previous submission, and were unchanged. They are consistent with the PFS reported in the IPASS trial for the pre-specified retrospectively determined EGFR M+ subgroup, showing a significant increase in PFS favouring gefitinib treatment:
- IPASS: median increase in PFS of 3.2 months (HR = 0.48 [95% CI 0.36, 0.64]);
- NEJ002: median increase in PFS of 5.4 months (HR = 0.30 [95% CI 0.22, 0.41]);
- WJTOG3405: median increase in PFS of 2.9 months (HR = 0.49 [95% CI 0.34, 0.71]).
A systematic review identified by the resubmission included a random effects model meta-analysis of the four trials comparing the effectiveness of gefitinib with platinum-based doublet chemotherapy in patients with EGFR M+ locally advanced or metastatic non-squamous NSCLC (Gao et al). The pooled hazard ratio supports the PFS results seen for the individual trials; it favours gefitinib treatment over chemotherapy (HR = 0.43 [95% CI 0.32, 0.58]) in EGFR M+ patients. Gao et al reported moderate heterogeneity between studies but this did not reach statistical significance (I2 = 57.8%, p = 0.07;). This is illustrated below.
The OS data were updated for both trials, but were still immature for the WJTOG3405 trial. As seen with the IPASS and First-SIGNAL trials, there was no significant difference between the two treatment arms in terms of OS (NEJ002 HR = 0.89 [95% CI 0.63, 1.24]; WJTOG3405 HR = 1.19 [95% CI 0.77, 1.83]).
The most common adverse events seen in the four main trials were consistent with the known safety profile of the treatments. Overall, the varying safety profiles of both treatment arms would require consideration in the context of an individual patient but gefitinib appeared to have less serious toxicity than platinum-based therapy.
The submission considered by the PBAC in November 2010 provided the gefitinib Periodic Safety Update Report (PSUR) covering the period from July 2008 to July 2009. This resubmission provided an updated PSUR from 12 February 2012, which covered the period from July 2011 to January 2012. The resubmission reported that the overall reporting rate of patients experiencing interstitial lung disease-type events was calculated at 2.13 per 100 patient years as of January 2012, with 71 cases reported, of which 21 described events with a fatal outcome. No new safety issues were identified.
For PBAC’s view, see Recommendations and Reasons.
9. Clinical Claim
The resubmission described EGFR mutation testing and treatment of EGFR M+ patients with gefitinib as superior in terms of PFS and non-inferior in terms of OS platinum-based doublet chemotherapy. The resubmission described gefitinib as superior in terms of comparative safety over platinum-based doublet chemotherapy. The PBAC considered that the clinical benefit of listing gefitinib as first-line treatment in addition to second-line treatment is an improvement in quality of life, but not a prolongation of life.
10. Economic Analysis
The resubmission presented an updated modelled economic evaluation (a cost-utility analysis in terms of cost per quality-adjusted life-year (QALY) gained) based on a superiority claim of the proposed scenario (both first-line EGFR testing and gefitinib are available) over the current scenario (neither first-line EGFR testing nor first-line gefitinib is available) for both comparative benefit and harms. The resubmission calculated an incremental cost-effectiveness ratio (ICER) in the range of $15,000 - $45,000/QALY based on the observed PFS benefit of first-line gefitinib over carboplatin with paclitaxel from the IPASS trial, extrapolated to 5 years (from a median follow-up of 17 months in the trial). Utility values were applied from quality of life scores reported in the IPASS trial that have been converted using an algorithm derived from another TKI (second-line) clinical trial (ZODIAC) as well as utility decrements associated with disease progression reported in one published study (Nafees et al. 2008).
The Product Information for gefitinib recommends periodic liver function testing. This was not included in the resource use in the economic analysis.
For PBAC’s view, see Recommendations and Reasons.
11. Estimated PBS Usage and Financial Implications
The likely number of patients per year, based on an assumption of 100% market share, was estimated in the submission to be less than 10,000 in Year 5, at an estimated net cost per year to the Government in the range of $10 -$30 million in Year 5.
For PBAC’s view, see Recommendation and Reasons.
12. Recommendation and Reasons
The PBAC accepted that the appropriate overall comparison, as reflected in the key IPASS randomised trial, was first-line chemotherapy with the option of alternative therapies, including erlotinib and gefitinib, after disease progression versus first-line gefitinib with the option of alternative therapies, including chemotherapy, after disease progression. The PBAC noted that the results of the smaller and under-powered First-SIGNAL trial were consistent with those of IPASS. The PBAC also accepted that gefitinib had advantages over chemotherapy in terms of its oral method of administration and its toxicity profile, noting that its duration of use was therefore not limited to a specific number of cycles of therapy.
The PBAC noted that the retrospectively identified subgroup in IPASS of EGFR test positive patients provided support to conclude that a statistically significant benefit existed for first-line gefitinib monotherapy over first-line platinum-based chemotherapy in terms of an additional median progression-free survival of 3.2 months (log rank p < 0.0001). The PBAC also noted from across the trial evidence that there was no improvement in overall survival for these patients. The PBAC therefore concluded that the clinical benefit for these patients of listing gefitinib as first-line treatment in addition to second-line treatment is an improvement in quality of life, but not a prolongation of life. In this regard, the PBAC rejected the argument presented in the pre-PBAC response that cross-over to TKI in EGFR positive patients explains increases in overall survival observed in patients randomised to chemotherapy in recent trials.
In contrast, the PBAC noted that, for the retrospectively identified subgroup in IPASS of EGFR test negative patients, the data showed a statistically significant worse outcome for first-line gefitinib monotherapy compared with first-line platinum-based chemotherapy for median progression-free survival, a reduction of 4.0 months (log rank p < 0.0001). The PBAC concluded that, because there are effective alternative therapies in the requested first-line setting, use of gefitinib in patients without an EGFR activating mutation would result in a net harm for patients. This establishes the need for EGFR testing before deciding whether to use gefitinib (because a minority of NSCLC patients test positive for EGFR activating mutations) and also established the importance of minimising false positive EGFR test results.
In relation to the importance of minimising false EGFR test results, the PBAC noted the discussion of the stakeholder meeting on EGFR testing and TKIs in NSCLC held on 18 October 2012. The PBAC accepted advice from the stakeholder meeting that a PBS restriction should not specify the specific EGFR activating mutations to allow experience to evolve, noting that the strongest evidence is limited to the EGFR mutations of exon 19 deletions and L858R point mutations on exon 21, which are estimated to account for about 70% of detected EGFR mutations. The PBAC also noted advice from the stakeholder meeting that an MBS item descriptor should allow all patients with NSCLC to be tested at initial diagnosis of NSCLC for histological subtype, and then for EGFR mutation status if not clearly having squamous cell carcinoma. This should occur at initial diagnosis with the tested specimen examined in one of a small number of pathology laboratories to ensure appropriate expertise and back-up. The PBAC therefore requested advice from MSAC as identified in the stakeholder meeting, especially about the implementation of optimal biopsy practice to obtain high rates of satisfactory specimens and implementation of optimal centralised pathology laboratory practice where the one site performs both histological and genetic testing. If this could be implemented, MSAC’s advice was also sought on whether this would provide sufficient confidence in the results of these tests to guide TKI treatment decisions.
The modelled economic evaluation compared current management, which involves first-line platinum-based chemotherapy without EGFR testing, with proposed management, which involves EGFR testing to guide first-line therapy to gefitinib or chemotherapy. As a result, the model’s estimated incremental QALY gain of 0.018 per patient is weighted across all patients tested and not limited to only those treated on the grounds of being EGFR test positive. The PBAC noted that the model, which extrapolated beyond the trial horizon to five years, appropriately limited the health outcome gains to quality of life improvements with gefitinib related to a prolonged time to progression of disease and a more favourable toxicity profile and did not include any improvement in overall survival.
However, the PBAC did not accept the Pre-PBAC response’s revised base case incremental cost effectiveness per extra QALY gained in the range of $45,000 - $75000/QALY for first-line gefitinib at its proposed price in the first-line setting. The PBAC noted that, although it appeared to satisfactorily resolve the issue with the ‘seed’ chosen to run the simulation, this new model had not been independently assessed, including in relation to the claim that it could satisfactorily assess the sensitivity of incremental ratio to uncertainty in the truth of EGFR test results. One concern with the model was that it assumed that the proportions of patients continuing on to second-line treatment were 60% for both arms and that this could not be varied across the arms in the sensitivity analyses. The analyses presented from the IPASS trial suggested that 47% of patients randomised to first-line chemotherapy received more expensive second-line TKIs and 73% of patients randomised to first-line gefitinib received cheaper second-line chemotherapy. Based on a sample of Medicare Australia data, 45% patients currently receiving first-line chemotherapy receive second-line therapy. Also, some patients randomised to gefitinib in the IPASS trial received a further TKI second-line or subsequently. The PBAC accepted advice from the Joint ESC meeting that there were other concerns with the model which favoured first-line gefitinib, such as the number of first-line chemotherapy cycles, the choice of chemotherapy drugs in the comparator arm, and inherent assumptions about optimal EGFR testing performance. The model might be more transparent if separate sub-models were developed for EGFR test positive and EGFR test negative patients, with separate results, which could be subsequently combined into a final model.
The financial implications are also uncertain, with an estimated net increased annual cost to government estimate in the range of $10 – 30 million in the fifth year of listing. The PBAC noted that a smaller off-set from reduced second-line TKI use was assumed in the financial analyses than in the economic evaluation
The PBAC therefore rejected the application to extend the listing of gefitinib, (at the proposed reduced price), to the first-line setting of locally advanced or metastatic NSCLC on the grounds of unacceptably high and uncertain cost-effectiveness, and noting also the expected lack of any overall survival gain for patients resulting from the proposed extended listing and that there is currently insufficient confidence in the accuracy of EGFR test results.
Given that the stakeholder meeting involved more than one TKI, the PBAC expressed a preference for a coordinated reconsideration of first-line treatment of locally advanced and metastatic NSCLC. This would need to address the varying and reducing costs of platinum-based chemotherapy where there is no differential health outcome basis associated with the different costs, and also the trend to earlier use of pemetrexed. This would also need to address the price advantage requested for gefitinib and erlotinib in this setting which is not justified by the extra QALYs gained, and which also needs to include the additional costs of identifying which patients are mutation positive. On a per treated patient basis at the proposed reduced price, first-line TKIs are proposed to cost between $19,000 and $20,000 per year compared with between $1,500 (carboplatin and gemcitabine) and $4,200 (carboplatin and paclitaxel) for four 3-week cycles of first-line chemotherapy, up to a maximum of $6,000 for six cycles of chemotherapy. Adding the costs of EGFR testing to identify eligible patients for a TKI further adds to the cost of this treatment option. The claimed cost off-sets and small QALYs gained are not sufficient to justify this cost differential at the prices requested for the TKIs.
The PBAC therefore also requested advice from MSAC, as identified at the stakeholder meeting and the Joint ESC advice, on the prevalence of EGFR mutations in Australian patients with NSCLC for pre-selected “enriched” population excluding squamous cell carcinoma; the number of tests per patient treated with first-line gefitinib, which should reflect the frequency of repeat testing under the proposed optimisation of biopsy practice (which varied by an order of magnitude between the economic evaluation [10%] and the financial analysis [1.2%]), and therefore the costs of testing per patient treated with first-line gefitinib; and the overall increase in the cost of testing to support first-line use compared with current testing for the existing PBS listing of gefitinib.
In the context of current knowledge about TKI therapy of NSCLC and the recent stakeholder meeting, the PBAC formed the view that future applications for gefitinib should consider a restriction to EGFR mutation positive patients but without specifying line of therapy. For the same reasons, alignment of gefitinib and erlotinib restrictions is clinically appropriate, so the existing second-line PBS listing of erlotinib would need to be re-considered and adjusted to restrict its availability on PBS to patients with an EGFR activating mutation.
The PBAC also acknowledged and noted the consumer comments on this item.
Recommendation:
Reject
13. Context for Decision
The PBAC helps decide whether and, if so, how medicines should be subsidised in Australia. It considers submissions in this context. A PBAC decision not to recommend listing or not to recommend changing a listing does not represent a final PBAC view about the merits of the medicine. A company can resubmit to the PBAC or seek independent review of the PBAC decision.
14. Sponsor’s Comment
AstraZeneca is committed to continuing efforts to seek equity of access for appropriately identified locally advanced or metastatic NSCLC patients in the first-line setting who are likely to benefit from gefitinib therapy.
