
Certolizumab Pegol, 200 mg/mL injection, 2 x 1 mL syringes, Cimzia® - March 2014
PDF printable version of this page
Public Summary Document
Product: Certolizumab Pegol, 200 mg/mL injection, 2 x 1 mL syringes, Cimzia®
Sponsor: UCB Australia Pty Ltd
Date of PBAC Consideration: March 2014
1. Purpose of Application
To request an Authority required listing for the treatment of adults with active ankylosing spondylitis (AS) who meet certain criteria.
2. Background
This was the first PBAC consideration of certolizumab pegol for AS.
At the March 2010 PBAC meeting, certolizumab was recommended for the treatment of rheumatoid arthritis on a cost-minimisation basis versus adalimumab.
3. Registration Status
The submission was made under TGA/PBAC Parallel Process. At the time of PBAC consideration, a positive ACPM Outcome was available.
As of 9 May 2014, certolizumab pegol was TGA registered for the following indications:
- Rheumatoid arthritis - indicated for the treatment of moderate to severe active rheumatoid arthritis (RA) in adult patients: combined with MTX in case of either an inadequate response or intolerance to previous therapy with one or more disease-modifying antirheumatic drugs (DMARDS) or: as monotherapy in case of a contraindication or intolerance to MTX.
- Psoriatic arthritis - indicated for the treatment of adult patients with active psoriatic arthritis where response to previous disease-modifying anti-rheumatic drug therapy (DMARDs) has been inadequate.
- Ankylosing Spondylitis - indicated for the treatment of adult patients with active, ankylosing spondylitis who have been intolerant to or have had inadequate response to at least one nonsteroidal anti-inflammatory drug (NSAID). Cimzia has been shown to improve physical function.
4. Listing Requested and PBAC’s View
Listing was requested for the treatment of adults with active ankylosing spondylitis who meet certain criteria. The restriction wording proposed was identical to the current PBS listing of etanercept, adalimumab and golimumab for active ankylosing spondylitis. The PBAC recommended the same restriction as for etanercept, adalimumab and golimumab for active ankylosing spondylitis apply to certolizumab.
The submission sought listing on a cost minimisation basis with adalimumab.
5. Clinical Place for the Proposed Therapy
The submission proposed that certolizumab would provide an alternative treatment option for ankylosing spondylitis to the currently available bDMARDs.
6. Comparator
Adalimumab was the primary comparator for the cost-minimisation analysis. Etanercept, infliximab and golimumab were nominated as secondary comparators. The PBAC considered the comparators to be appropriate.
7. Clinical Trials
The submission did not present any direct head-to-head trials comparing certolizumab to adalimumab (or any other bDMARD). The submission was based on an indirect comparison of trials as follows; one trial comparing certolizumab to placebo (AS001), three trials comparing adalimumab to placebo (Canadian-AS, ATLAS and Huang 2013), five trials comparing etanercept to placebo (Davis 2003, Calin 2004, Wyeth Study, Barkham 2010 and SPINE), two trials comparing infliximab to placebo (Braun 2002 and ASSERT), and two trials comparing golimumab with placebo (GO RAISE and Bao 2012).
Details of the trials and associated reports presented in the submission are in the table below.
|
Trial |
Protocol title/ Publication title |
Publication citation |
|---|---|---|
|
Certolizumab versus placebo |
||
|
AS001 |
AS001 Clinical study report. Randomised, double-blind, parallel-group, placebo-controlled study to evaluate efficacy and safety of CZP in adult subjects with active AxSpa |
25 January 2013 |
|
Landewé R, Braun J, Deodhar A, et al. Efficacy of certolizumab pegol on signs and symptoms of axial spondyloarthritis including ankylosing spondylitis: 24-week results of a double-blind randomised placebo-controlled Phase 3 study. |
Ann Rheum Dis. Online First: 6 Sep 2013 |
|
|
Adalimumab versus placebo |
||
|
Canadian-AS |
Lambert R, Salonen D, Rahman P, et al. Adalimumab significantly reduces both spinal and sacroiliac joint inflammation in patients with ankylosing spondylitis. (2007) |
Arthritis Rheum 2007; 56(12):4005-4014. |
|
Maksymowch W, Rahman P, Keystone E, Wong R and Inman R. Efficacy of adalimumab in active ankylosing spondylitis (AS) - Results of the Canadian AS study. |
Arthritis Rheum 2005; 52(9):S217.Abstract No.505. |
|
|
Maksymowych WP, Rahman P, Shojania K, et al. Beneficial effects of adalimumab on biomarkers reflecting structural damage in patients with ankylosing spondylitis. |
Journal of Rheumatology 2008; 35(10):2030-2037. |
|
|
ATLAS |
Van der Heijde D, Kivitz A, Schiff M, et al. Efficacy and safety of adalimumab in patients with ankylosing spondylitis: Results of a multicenter, randomized, double-blind, placebo-controlled trial. |
Arthritis Rheum 2006; 54(7):2136-2146. |
|
Huang 2013 |
Huang et al. Efficacy and safety of adalimumab in Chinese adults with active ankylosing spondylitis: results of a randomised, controlled trial |
Ann Rheum Dis. ePub ahead of print March 8, 2013. |
|
Etanercept versus placebo |
||
|---|---|---|
|
Davis 2003 |
Davis Jr JC, van der Heijde D, Braun J, Dougados M, Cush J, Clegg DO et al. Recombinant Human Tumor Necrosis Factor Receptor (Etanercept) for Treating Ankylosing Spondylitis: A Randomised, Controlled Trial. |
Arthritis & Rheumatism 2003; 48(11): 3230-6. |
|
Davis J, van der Heijde D, Dougados M, et al. Baseline factors that influence ASAS20 response in patients with ankylosing spondylitis treated with etanercept. |
Journal of Rheumatology 2005; 32(9):1751-1754. |
|
|
Calin 2004 |
Calin A, Dijkmans B, Emery P, et al. Outcomes of a multicentre randomised clinical trial of etanercept to treat ankylosing spondylitis. |
Ann Rheum Dis 2004; 63(12):1594-1600. |
|
Dijkmans B, Emery P, Hakala M, et al. Etanercept in the long term treatment of patients with ankylosing spondylitis. |
Journal of Rheumatology 2009; 36(6):1256-1264. |
|
|
Wyeth Study |
Van der Heijde D, Da Silva J, Dougados M, et al. Etanercept 50 mg once weekly is as effective as 25 mg twice weekly in patients with ankylosing spondylitis. |
Ann Rheum Dis 2006; 65:1572-1577. |
|
Barkham 2010 |
Barkham N, Coates LC, Keen H, Hensor E, Fraser A, Redmond A, Cawkwell L, Emery P. Double-blind placebo-controlled trial of etanercept in the prevention of work disability in ankylosing spondylitis. |
Ann Rheum Dis 2010; 69(11):1926-8. |
|
SPINE |
Dougados M et al. Efficacy of etanercept on rheumatic signs and pulmonary function tests in advanced ankylosing spondylitis: results of a randomised double-blind placebo-controlled study (SPINE) |
Ann Rheum Dis. 2011; 70:799–804. |
| Infliximab versus placebo | ||
|
Braun 2002 |
Braun J, Brandt J, Listing J, Zink A, Alten R, Golder W et al. Treatment of active ankylosing spondylitis with infliximab: a randomised controlled multi-centre trial. |
Lancet 2002; 359(9313): 1187-93. |
|
ASSERT |
Van Der Heijde D, Dijkmans B, Geusens P, et al. Efficacy and safety of infliximab in patients with ankylosing spondylitis: Results of a randomized, placebo-controlled trial (ASSERT). |
Arthritis and Rheumatism 2005; 52:582-591. |
| Golimumab versus placebo | ||
|
GO RAISE |
Inman RD, Davis J, Van Der Heijde D, et al. Efficacy and safety of golimumab in patients with ankylosing spondylitis: Results of a randomised, double-blind, placebo-controlled, phase III trial. |
Arthritis and Rheumatism 2008; 58(11):3402-3412. |
|
Bao 2012 |
Bao et al. Golimumab Administered Subcutaneously Every 4 Weeks in Chinese Patients with Active Ankylosing Spondylitis: Week 24 Safety and Efficacy Results From a Randomized, Placebo-Controlled Study |
Arthritis and Rheumatism 2012; 64 SUPPL. 10 (S589) |
The key features of the trials included in the indirect comparison and their previous consideration by the PBAC are outlined in the table below.
|
Trial |
N |
Design / duration |
Bias risk |
Patient population |
Previously considered by PBAC |
|---|---|---|---|---|---|
|
CZP v PLA |
|||||
|
AS001 |
325# |
R, DB, 3A ESC, 24wk |
Low/ Unclear |
axSpA; TNFα naïve and experienced |
No |
|
ADA v PLA |
|||||
|
Canadian-AS |
82 |
R, DB, 2A, 24wk |
Low |
AS; TNFα naïve |
ADA (Nov 06) GOL (Mar 10) |
|
ATLAS |
315 |
R, DB, 2A ESC, 24wk |
Low |
AS; TNFα naïve |
|
|
Huang 2013 |
344 |
R, DB, 2A, 24wk |
Low |
AS; TNFα naïve |
No |
|
ETC v PLA |
|||||
|
Davis 2003 |
277 |
R, DB, 2A, 24wk |
Low |
AS; TNFα naïve |
ETC (Jul 04) ADA (Nov 06) GOL (Mar 10) |
|
Calin 2004 |
84 |
R, DB, 2A, 12wk |
Low |
AS; TNFα naïve |
|
|
Wyeth study |
356 |
R, DB, 3A, 12wk |
Low |
AS; TNFα naïve |
GOL (Mar 10) |
|
Barkham 2010 |
40 |
R, DB, 2A, 12wk |
Low |
AS; TNFα naïve |
No |
|
SPINE |
82 |
R, DB, 2A, 12wk |
Low |
AS; TNFα naïve |
No |
|
INF v PLA |
|||||
|
Braun 2002 |
69 |
R, DB, 2A, 12wk |
Low |
AS; TNFα naïve |
INF (Dec 03) ETC (Jul 04) GOL (Mar 10) |
|
ASSERT |
279 |
R, DB, 2A, 24wk |
Low |
AS; TNFα naïve |
GOL (Mar 10) |
|
GOL v PLA |
|||||
|
GO RAISE |
356 |
R, DB, 3A ESC, 24wk |
Low |
AS; TNFα naïve |
GOL (Mar 10) |
|
Bao 2012 |
213 |
R, DB, 2A ESC, 48wk |
Low |
AS; TNFα naïve |
No |
Abbreviations: CZP=certolizumab; ADA=adalimumab; ETC=etanercept; INF=infliximab; GOL=golimumab; PLA=placebo; DB=double blind; R=randomised; A=arm; ESC=escape regimen (for placebo); AS=ankylosing spondylitis; axSpA=axial spondoarthritis; TNFα=tumour necrosis factor alpha (inhibitor);
# n=178 for AS subgroup
The PBAC noted there were no consumer comments on this item. The PBAC noted there was no hearing for this item.
8. Results of Trials
The submission nominated a non-inferiority margin of a 20% improvement in the Assessment in AS working group (ASAS20) at Week 12. Certolizumab was considered non-inferior in the indirect comparison if the 95% CI of the relative risk in the ASAS20 response included the value 1.00 and the lower bound of the 95% CI was greater than 0.43. The ASAS20 was the primary outcome in the certolizumab versus placebo trials and the adalimumab versus placebo trials.
The table below presents the results for the ASAS20 outcome, measured at 12 weeks in all trials with the exception of the golimumab trials (Bao 2012 and GO-RAISE), in which the ASAS20 was measured at 14 weeks.
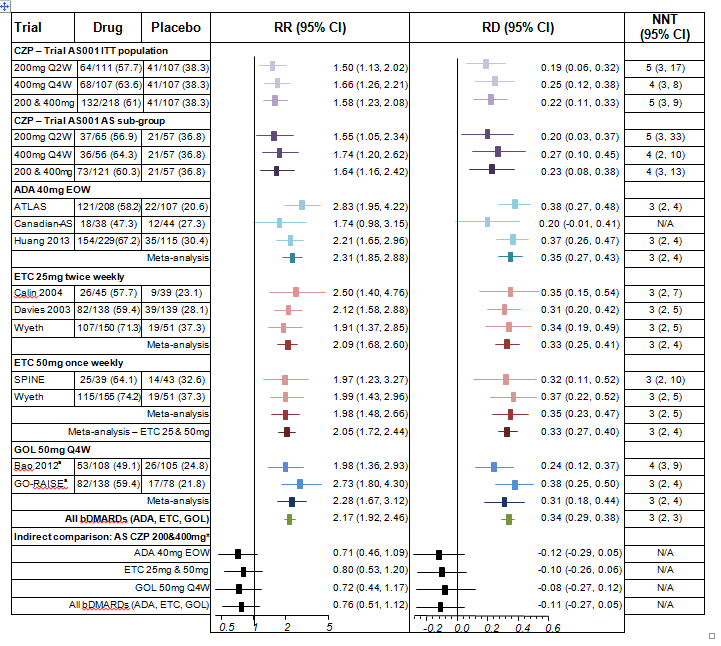 Abbreviations: CZP=certolizumab; ADA=adalimumab; ETC=etanercept; GOL=golimumab.
Abbreviations: CZP=certolizumab; ADA=adalimumab; ETC=etanercept; GOL=golimumab.
AS subgroup, Certolizumab 200mg Q2W v 400mg Q4W: RR=0.89 (0.66, 1.19) RD=-0.07 (-0.24, 0.10)
Etanercept 25mg twice weekly v 50mg once weekly: RR=0.96 (0.60, 1.54); RD=-0.02 (-0.16, 0.12)
All meta-analyses conducted using a random effects model
a Results at week 14
The PBAC noted that all trials demonstrated that active treatments resulted in a statistically significantly greater proportion of patients achieving a 20% improvement in the ASAS score (ASAS20) compared with placebo at week 12 or 14, with the exception of the Canadian-AS trial (adalimumab versus placebo).
The PBAC considered that the indirect comparisons indicated there were no statistically significant difference between certolizumab and any of the bDMARDs or the combined bDMARDs and that the nominated non-inferiority criterion of 0.43 was satisfied in all indirect comparisons.
A 50% improvement in the Bath Ankylosing Spondylitis Disease Activity Index score (BASDAI50) was measured at 12 weeks in all trials with the exception of the golimumab trial (GO-RAISE), which was measured at 14 weeks. All trials demonstrated that the active treatments resulted in a statistically significantly greater proportion of patients achieving a BASDAI50 compared with placebo at week 12 or 14. The indirect comparisons indicated there were no statistically significant difference between certolizumab and any of the bDMARDs or the combined bDMARDs.
The results for ASAS20 at Week 24 were consistent with the results presented at week 12/14.
The submission presented a summary of adverse events reported in the total safety population for the 24-week double blind period in AS001. The table below presents this summary with safety data for the placebo-escape patients included in the “All CZP” group (and not included in the placebo group).
|
|
PLA |
CZP 200 |
CZP 400 |
200+400 |
All CZP |
RR (95% CI)a |
|---|---|---|---|---|---|---|
|
N=107 |
N=111 |
N=107 |
N=218 |
N=274 |
All CZP v PLA |
|
|
Any TEAEs |
67 (63) |
85 (77) |
80 (75) |
165 (76) |
193 (70) |
1.12 (0.95, 1.33) |
|
Severe TEAEs |
7 (7) |
4 (4) |
3 (3) |
7 (4) |
10 (4) |
0.56 (0.22, 1.43) |
|
DR-TEAEs *** |
22 (21) |
41 (37) |
36 (34) |
77 (35) |
91 (33) |
1.62 (1.07, 2.43) |
|
Serious TEAEs |
5 (5) |
4 (4) |
7 (7) |
11 (6) |
13 (5) |
1.02 (0.37, 2.78) |
|
Disc. due to TEAEs |
2 (2) |
2 (2) |
4 (4) |
6 (3) |
6 (2) |
1.17 (0.24, 5.71) |
|
AE leading to death |
0 (0) |
0 (0) |
0 (0) |
0 (0) |
0 (0) |
- |
|
TEAEs |
||||||
|
Infections |
25 (23) |
43 (39) |
41 (38) |
84 (38) |
95 (35) |
1.48 (1.02, 2.17) |
|
Serious infections |
0 (0) |
2 (2) |
0 |
2 (2) |
3 (1) |
2.75 (0.14, 52.78) |
|
Nasopharyngitis |
7 (7) |
11 (10) |
11 (10) |
22 (10) |
24 (9) |
1.34 (0.59, 3.01) |
|
Pharyngitis |
1 (1) |
5 (5) |
1 (1) |
6 (6) |
7 (3) |
2.73 (0.34, 21.95) |
|
URTI |
3 (3) |
6 (5) |
4 (4) |
10 (5) |
11 (4) |
1.43 (0.41, 5.03) |
|
Inj. site reactions |
1 (1) |
10 (9) |
5 (5) |
15 (7) |
18 (7) |
7.03 (0.95, 52.0) |
|
Elevated blood CPK |
2 (2) |
7 (6) |
6 (6) |
13 (6) |
14 (5) |
2.73 (0.63, 11.83) |
|
Headache |
7 (7) |
7 (6) |
9 (8) |
16 (7) |
17 (6) |
0.95 (0.40, 2.22) |
|
Rash |
2 (2) |
3 (3) |
4 (4) |
7 (4) |
12 (4) |
2.34 (0.53, 10.29) |
Abbreviations: TEAE=treatment emergent adverse event; DR=drug-related; AE=adverse event; CPK=creatinine phosphokinase; UTRI=upper respiratory tract infection
a given approximately half placebo patients (56/107) escaped to active at week 16, of approximately half (56/107), the comparisons are biased.
The PBAC noted that the treatment emergent adverse events (TEAEs) were mostly mild or moderate in severity and not considered treatment related. The most common infections were nasopharyngitis (9% v 7%) and upper respiratory tract infections (4% v 3%). For non-infection AEs, headache and increased blood creatinine phosphokinase were most common. A similar pattern of TEAEs was observed in the AS subgroup of patients.
The submission provided additional data on potential safety concerns beyond those identified in the clinical trials based on;
- The broader clinical trial program for CZP;
- A literature search; and
- The sixth Periodic Safety Update Report (PSUR).
Based on the evidence presented, the PBAC accepted that the safety profile of certolizumab appeared to be consistent with the known safety profiles of the other bDMARDs for the treatment of AS.
A summary of the comparative benefits and harms for certolizumab versus adalimumab are presented in the table below.
|
Trial |
N (1) |
RR (95%CI) |
Event rate/100 patients/year |
Increment |
|
|
Druga |
Placebo |
||||
|
Benefits - ASAS20 at week12/14 |
|||||
|
Certolizumab 200&400mg |
|||||
|
ITT |
1 (325) |
1.58 (1.23, 2.08) |
61 |
38.3 |
22 (11, 33) |
|
AS sub-group |
1 (178) |
1.64 (1.15, 2.42) |
60.3 |
36.8 |
23 (8, 38) |
|
Adalimumab 40mg EOW |
|||||
|
ATLAS |
1 (315) |
2.83 (1.95, 4.22) |
58.2 |
20.6 |
38 (27, 48) |
|
Canadian-AS |
1 (82) |
1.74 (0.98, 3.15) |
47.3 |
27.3 |
NS |
|
Huang 2013 |
1 (344) |
2.21 (1.65, 2.96) |
67.2 |
30.4 |
37 (26, 47) |
|
Meta-analysis |
3 (741) |
2.31 (1.85, 2.88) |
61.7 |
25.9 |
35 (27, 43) |
|
Indirect comparison of certolizumab 200&400mg (AS sub-group) and adalimumab 40mg EOW |
|||||
|
|
N (1) |
RR (95%CI) |
Certolizumabb |
Adalimumabb |
Increment |
|
4 (919) |
0.71 (0.46, 1.09) |
22 |
35 |
NS |
|
Abbreviations: EOW=every other week; NS=not significant
a certolizumab or adalimumab (comparator used for the cost-minimisation analysis)
b incremental event rate compared to placebo
9. Clinical Claim
The submission claimed that certolizumab is non-inferior in terms of comparative effectiveness and safety to adalimumab, etanercept, infliximab and golimumab. Based on the evidence presented and the nominated non-inferiority criterion the PBAC accepted these claims.
10. Economic Analysis
The submission presented a cost-minimisation analysis. The proposed equi-effective doses of certolizumab and adalimumab for AS were based on the indirect comparisons presented in the submission. The doses are identical to the established therapeutic relativities between the agents for rheumatoid arthritis on the PBS, and are outline in the table below.
|
Indication |
Non-inferior / equivalence doses |
Source |
|
|
CZP |
ADA |
||
|
RA |
400mg at 0,2,4 followed by 200mg q2w or 400mg q4w |
40mg q2w |
Therapeutic relativity sheets October 2010 |
|
AS |
400mg at 0,2,4 followed by 200mg q2w or 400mg q4w |
40mg q2w |
Indirect analysis (see Section B.6) |
Abbreviations: CZP=certolizumab; ADA=adalimumab; RA=rheumatoid arthritis; AS=ankylosing spondylitis; q2w=every 2 weeks; q4w=every 4 weeks
The submission presented a cost analysis of the certolizumab 200mg maintenance regimen over a two year period at the requested price (DPMQ) compared with adalimumab. The cost-analysis was updated during the evaluation to (also) include the certolizumab 400mg regimen (assuming 50:50 prescribing of the two regimens).
The PBAC noted that the cost analysis resulted in certolizumab being cost neutral to adalimumab only for the 400 mg maintenance regimen.
The PBAC accepted the presented cost analysis approach that was based on a two year time period, with a price based on certolizumab’s price for rheumatoid arthritis.
The PBAC recommended that certolizumab for AS be listed on a cost minimisation basis with adalimumab.
11. Estimated PBS Usage and Financial Implications
The likely number of certolizumab pegol prescriptions per year was estimated in the submission to be less than 10,000 in Year 5, at an estimated net cost per year to the PBS of less than $1 million in Year 5.
The PBAC noted that the financial implications were most sensitive to the market uptake assumptions. Should certolizumab achieve equal market uptake as golimumab achieved after its listing in 2010 for AS, the net cost to the government over 5 years would be higher than estimated.
12. Recommendation and Reasons
The PBAC recommended the extending the authority required listing of certolizumab pegol to include the treatment of active ankylosing spondylitis (AS) in patients who meet certain criteria on a cost minimisation basis with adalimumab. The equi-effective doses are 400 mg certolizumab at weeks zero, two and four, then 200 mg every two weeks or 400 mg every four weeks, and adalimumab 40 mg every two weeks.
The PBAC recommended the same restriction as for etanercept, adalimumab and golimumab for active ankylosing spondylitis apply to certolizumab. The PBAC agreed that certolizumab would provide an alternative treatment option for ankylosing spondylitis to the currently available bDMARDs.
Adalimumab was the primary comparator for the cost-minimisation analysis. Etanercept, infliximab and golimumab were nominated as secondary comparators. The PBAC considered the comparators to be appropriate.
The submission did not present any direct head-to-head trials comparing certolizumab to adalimumab (or any other bDMARD). The submission was based on an indirect comparison of trials as follows; one trial comparing certolizumab to placebo (AS001), three trials comparing adalimumab to placebo (Canadian-AS, ATLAS and Huang 2013), five trials comparing etanercept to placebo (Davis 2003, Calin 2004, Wyeth Study, Barkham 2010 and SPINE), two trials comparing infliximab to placebo (Braun 2002 and ASSERT), and two trials comparing golimumab with placebo (GO RAISE and Bao 2012). The PBAC noted that all trials demonstrated that the active treatments resulted in a statistically significantly greater proportion of patients achieving a 20% improvement in the ASAS score (ASAS20) compared with placebo at week 12 or 14, with the exception of the Canadian-AS trial (adalimumab versus placebo).
The PBAC considered that the indirect comparisons indicated there were no statistically significant difference between certolizumab and any of the bDMARDs or the combined bDMARDs and that the nominated non-inferiority criterion of 0.43 was satisfied in all indirect comparisons.
The submission presented a summary of adverse events reported in the total safety population for the 24-week double blind period in AS001. The submission also provided additional data on potential safety concerns beyond those identified in the clinical trials based on the broader clinical trial program for certolizumab, a literature search and the sixth Periodic Safety Update Report. Based on the evidence presented the PBAC agreed that the safety profile of certolizumab appeared to be consistent with the known safety profiles of the other bDMARDs for the treatment of AS.
Based on the evidence presented and the nominated non-inferiority criterion the PBAC considered certolizumab to be non-inferior in terms of comparative efficacy and safety to adalimumab, etanercept, infliximab and golimumab.
The submission presented a cost-minimisation analysis. The proposed equi-effective doses of certolizumab and adalimumab for AS were based on the indirect comparisons presented in the submission, and the requested price of certolizumab for ankylosing spondylitis was the price of certolizumab for rheumatoid arthritis. The cost analysis was based on certolizumab 200 mg maintenance regimen over a two year period at the requested price (DPMQ) compared with adalimumab. The cost-analysis was updated during the evaluation to (also) include the certolizumab 400 mg regimen (assuming 50:50 prescribing of the two regimens). The PBAC noted that the cost analysis resulted in certolizumab being cost neutral to adalimumab only for the 400 mg maintenance regimen.
The PBAC considered that the cost analysis approach presented, that was based on a two year time period with a price based on certolizumab’s price for rheumatoid arthritis was acceptable, and recommended that certolizumab for AS be listed on a cost minimisation basis with adalimumab.
In accordance with subsection 101(3BA) of the National Health Act 1953, the PBAC advised that it is of the opinion that, on the basis of the material available to it at its March 2014 meeting, certolizumab should be treated as interchangeable with etanercept, adalimumab, golimumab and infliximab on an individual patient basis.
Recommendation:
Recommended.
Restriction to be finalised
13. Context for Decision
The PBAC helps decide whether and, if so, how medicines should be subsidised in Australia. It considers submissions in this context. A PBAC decision not to recommend listing or not to recommend changing a listing does not represent a final PBAC view about the merits of the medicine. A company can resubmit to the PBAC or seek independent review of the PBAC decision.
14. Sponsor’s Comment
The sponsor has no comment.

