
Voriconazole, 50 mg tablet, 56, 200 mg tablet, 56 and 40 mg/mL oral liquid: powder for, 70 mL, Vfend®, Pfizer Australia Pty Ltd
PDF printable version of this page
1 Purpose of Application
The major submission sought to extend the current Authority required listings of voriconazole to include the prophylaxis against invasive fungal infections in patients at high risk of developing such infections.
2. Requested listing
2.1 The submissions proposed new indication is shown below.
|
Name, Restriction, Manner of administration and form |
Max Qty |
No. of Rpts |
|
Proprietary Name and Manufacturer |
|
|---|---|---|---|---|---|
|
Voriconazole Tablet 50 mg Tablet 200 mg Powder for suspension 40mg/ml for 70ml oral liquid
|
56 56 1 |
2 2 0 |
|
Vfend Vfend Vfend |
PF PF PF |
|
Indication: |
Prophylaxis of invasive fungal infections, including both yeasts and moulds, in a patient who is at high risk of developing these infections. |
|---|---|
|
Treatment Phase: |
Initial |
|
Restriction: |
Authority Required |
|
Clinical criteria: |
High risk patient groups are defined as: (1) Acute myeloid leukaemia (AML) or high-risk myelodysplastic syndrome (MDS) Patient with anticipated neutropenia (an absolute neutrophil count of less than 500 cells per cubic millimetre) for at least 10 days, who are receiving chemotherapy for acute myeloid leukaemia or myelodysplastic syndrome. Treatment should continue until recovery of the neutrophil count to at least 500 cells per cubic millimetre. Patients who have had a previous invasive fungal infection should have secondary prophylaxis during subsequent episodes of neutropenia. (2) Graft versus host disease (GVHD) Patients with acute GVHD grades II to IV or extensive chronic GVHD, who are receiving intensive immunosuppressive therapy after allogeneic haematopoietic stem cell transplant. No more than 6 months therapy per episode will be PBS-subsidised. (3) High risk allogeneic haematopoietic stem cell transplant (AlloHSCT) recipients High risk AlloHSCT can be defined as neutropenia phase, cord blood, unrelated donor transplant with bone marrow stem cell source or likely delayed engraftment. No more than 6 months therapy per episode will be PBS-subsidised. |
2.2 Listing was sought on a cost minimisation basis against a mix of posaconazole fluconazole and itraconazole as the comparators.
2.3 It was noted that the proposed restriction did not meet current electronic media requirements and that the existing restrictions for the other indications would have to be remodelled to meet current electronic media requirements. This may potentially delay implementation of the change to the listings.
2.4 There was initially some ambiguity in the submission’s definition of patient groups at ‘high risk’ which the ESC sought to clarify The PBAC accepted the ESC’s clarification. The definitions of the three requested groups for whom the submission was seeking subsidy for prophylaxis with voriconazole were as follows:
Patient groups at high risk of invasive fungal infections are defined as:
1) Acute myeloid leukaemia (AML) or high-risk myelodysplastic syndrome (MDS).
Patients with anticipated neutropenia (an absolute neutrophil count less than 500 cells per cubic millimetre) for at least 10 days who are receiving chemotherapy for acute myeloid leukaemia or myelodysplastic syndrome.
2) Graft versus host disease (GVHD)
Patients with acute GVHD grades II to IV or extensive chronic GVHD who are receiving intensive immunosuppressive therapy after allogeneic haematopoietic stem cell transplant. (No more than 6 months therapy per episode will be PBS-subsidised).
3) High risk allogeneic haematopoietic stem cell transplant (AlloHSCT) recipients.
High risk AlloHSCT can be defined as neutropenia phase in: cord blood; unrelated donor transplant with bone marrow stem cell source; or likely delayed engraftment. (No more than 6 months therapy per episode will be PBS-subsidised).
2.5 The PBAC considered that for the AlloHSCT patient population, given that engraftment usually occurs in up to 30 days post-transplant or longer (up to 42 days) in some patients, provision for up to 2 months of treatment would be reasonable. For the other two groups (AML/MDS and GVHD), up to 6 months’ therapy per Authority prescription may be appropriate in some patients. The PBAC therefore recommended zero repeats for the listing, with the expectation that prescribers would request the appropriate number of repeats for their patient at the time of the Authority approval.
3 Background
3.1 Voriconazole (oral and IV formulations) has been registered with the TGA since 13 September 2002 for treatment of fungal infections. The indication for prophylactic use in patients at high risk of invasive fungal infections was TGA approved on 11 January 2013.
3.2 Voriconazole oral and IV formulations were recommended for PBS listing for treatment indications at the June 2003 PBAC meeting.
3.3 This was the first consideration by the PBAC of voriconazole for prophylaxis in patients at high risk of invasive fungal infections.
4 Clinical place for the proposed therapy
4.1 Voriconazole would provide an alternative option to the main comparator posaconazole for the prophylaxis of invasive fungal infections in high-risk AML/MDS and GVHD populations. Voriconazole would be the only drug available on the PBS for high-risk AlloHSCT patients if recommended by the PBAC.
5 Comparator
5.1 Posaconazole 200 mg three times daily was nominated as the main comparator. The submission also included fluconazole and itraconazole as secondary comparators. The PBAC accepted posaconazole as the appropriate main comparator.
6 PBAC consideration of the evidence
Consumer comments and sponsor hearing
6.1 The PBAC noted that no consumer comments were received for this item.
6.2 The PBAC noted that the sponsor did not request a hearing for this item.
Clinical trials
6.3 In the absence of head-to-head trials, the submission presented an indirect comparison, using fluconazole and itraconazole as common comparators. Direct (supplementary) evidence was provided as trials comparing voriconazole and itraconazole/fluconazole; and also observational studies comparing voriconazole and posaconazole. The submission presented the available evidence in two groups on the basis of disease type – the haemopoetic stem cell transplant (HSCT) at risk of GVHD population, and AML/MDS population. The trials and studies presented in the submission are shown in the table below.
|
Trial ID/First author |
Protocol title/ Publication title |
Publication citation |
|---|---|---|
|
HSCT/GVHD – indirect comparison voriconazole vs. posaconazole; common comparator fluconazole |
||
|
Wingard |
Randomized, double-blind trial of fluconazole versus voriconazole for prevention of invasive fungal infection after allogeneic hematopoietic cell transplantation. |
Blood 2010; 116(24):5111-8 |
|
Gergis |
Voriconazole provides effective prophylaxis for invasive fungal infection in patients receiving glucocorticoid therapy for GVHD. |
Bone Marrow. 2010; 45:662-667 |
|
Ullmann |
Posaconazole or Fluconazole for Prophylaxis in Severe Graft-versus-Host Disease. |
N Engl J Med. 2007; 356:335-347 |
|
AML/MDS population – common reference itraconazole |
||
|
Mattiuzzi |
Efficacy and safety of intravenous voriconazole and intravenous itraconazole for antifungal prophylaxis in patients with acute myeloid leukaemia or high-risk myelodysplastic syndrome. |
Support Care Cancer. 2011; 19(1):19-26. |
|
|
|
|
|
(Supplementary) direct evidence: Trials and studies comparing voriconazole and itraconazole/fluconazole; observational studies comparing voriconazole and posaconazole |
||
|
Randomised trial |
||
|
A1501073 |
Prospective, open-label, comparative, multicenter Study of voriconazole compared to itraconazole for the primary prophylaxis of invasive fungal infections (IFI) in subjects with allogeneic hematopoietic stem cell transplants (HSCT).
|
Internal clinical study report A1501073, 2010.
|
|
Marks |
Voriconazole versus itraconazole for antifungal prophylaxis following allogeneic haematopoietic stem-cell transplantation. |
British Journal of Haematology. 2011; 155(3):318-27 |
|
Observational studies |
||
|
Ananda-Rajah |
Comparative clinical effectiveness of prophylactic voriconazole/posaconazole to fluconazole/itraconazole in patients with acute myeloid leukaemia/ myelodysplastic syndrome undergoing cytotoxic chemotherapy over a 12-year period.
|
Haematologica. 2012; 97(3):459-63. |
|
Ojeda-Uribe |
Results of a prospective non-randomised trial comparing the efficacy of voriconazole and posaconazole as primary prophylactic agents of invasive fungal infections in acute leukemic patients.
|
Blood. 2011;118: Abstract 1120 |
|
Wetzstein |
Comparable efficacy and safety with voriconazole or posaconazole as primary antifungal prophylaxis in acute myeloid leukaemia patients receiving induction chemotherapy. |
Blood. 2009;114: Abstract 2059 |
Comparative effectiveness
6.4 For the indirect comparison between voriconazole and posaconazole, the submission presented the following outcome measures:
- Incidence of proven or probable invasive fungal infection. This outcome measure was reported in all of the randomised trials (primary outcome: Ullmann 2007, Mattiuzzi 2011 and Cornely 2007; secondary outcome: Wingard 2010) and the non-randomised study (secondary outcome: Gergis 2010)
- Mortality rate (all-cause). This outcome measure was reported in all of the randomised trials as a secondary outcome. Gergis 2010 reported incidence of invasive fungal infection related mortality and overall survival at 100 days from initiation of glucocorticoid therapy.
6.5 The time period over which incidence of invasive fungal infection was assessed varied across the trials and studies in the HSCT/GVHD population (Wingard 2010: 180 days post-transplant; Gergis 2010: 100 days from initiation of glucocorticoid therapy; Ullmann 2007: randomisation to day 112). In the AML/MDS population, incidence of invasive fungal infection was assessed over the prophylactic treatment phase. Also, across the trials there were differences in approaches to the identification of invasive fungal infections.
6.6 Results of the indirect comparisons across the various trials for the primary outcome of incidence of proven or probable invasive fungal infection are shown in the table below.
|
Trial ID |
VORI |
ITRA |
FLUC |
POSA |
RD % (95% CI) |
RR* (95% CI) |
|---|---|---|---|---|---|---|
|
HSCT/ GVHD |
||||||
|
Wingard 2010 |
14/305 (4.6%) |
- |
24/295 (8.1%) |
- |
-3.55 (-7.71, 0.37) |
0.56 (0.30, 1.06) |
|
Gergis 2010 |
2/97 (2.1%) |
7/72 (9.7%) |
-7.66 (-16.95, -0.88) |
0.21 (0.05, 0.87) |
||
|
Ullmann 2007 |
- |
27/299 (9.0%) |
16/301 (5.3%) |
-3.71 (-8.06, 0.43) |
0.59 (0.33, 1.06) |
|
|
Wingard 2010 vs. Ullmann 2007 |
0.17 (-5.69, 6.03) |
0.96 (0.40, 2.27) |
||||
|
Gergis 2010 vs. Ullmann 2007 |
-3.95 (-13.03, 5.14) |
0.36 (0.08, 1.67) |
||||
6.7 Results of the indirect comparison for the outcome of all-cause mortality showed no statistically significant difference between voriconazole and fluconazole. The PBAC agreed with the ESC that there were a number of factors that made the comparison of the clinical trials difficult to interpret and therefore the submission’s clinical claim of non-inferiority to posaconazole in terms of invasive fungal infections averted and all-cause mortality, not well supported. These factors included:
- The considerable differences between the risk categorisation of people with AlloHSCT in the Wingard trial (wide variability in risk) compared to Ullmann (higher risk group).
- The high risk of bias and confounding present in the Gergis 2010 observational study.
- Whether the populations in the trials and observational studies adequately represented the high-risk allogenic haemopoietic stem cell transplant (AlloHSCT) patients as requested in the PBS listing. AlloHSCT patients in Wingard 2010 were not recruited on the basis of having a cord blood or unrelated donor transplant with bone marrow stem cell source or increased likelihood of delayed engraftment.
- The intravenous (IV) formulation of voriconazole used in Mattiuzzi 2011 and whether it could be assumed that the same results would be achieved with oral voriconazole formulations.
6.8 Notwithstanding these factors, based on the results of the indirect comparisons, the PBAC considered it likely that voriconazole is non-inferior to posaconazole in terms of fungal infections averted and in preventing all-cause mortality
Comparative harms
6.9 The PBAC noted that a formal comparison of safety between voriconazole and posaconazole in the prophylactic setting was not provided due to the limited availability of data. The submission relied on a qualitative comparison of adverse events across the different trials, presenting adverse events from Trial A1501073, Wingard 2010, Mattiuzzi 2011, Ullmann 2007 and Cornely 2007. The pre-sub-committee response claimed that the Ullmann 2007 and Trial A1501073 provide the best safety data for comparison.
6.10 In addition to the lack of a direct comparison for safety outcomes, the PBAC noted the high rate of treatment-related visual impairment reported in A1501073, and, concerns of photosensitive rash and hepatobiliary adverse events. The pre-PBAC response noted that all reported visual impairment cases were mild to moderate in severity and that these effects are reversible.
6.11 Although the claim of non-inferior safety was not well supported against the nominated main comparator, posaconazole due to the absence of a statistical comparison of safety in this submission, the PBAC recalled that it had previously considered that the safety profile for posaconazole is comparable to that of fluconazole/itraconazole, noting that this consideration was made on the basis of adverse events reported in Ullmann 2007 and Cornely 2007. The PBAC considered it likely that voriconazole’s safety profile is similar to other azole antifungals.
Clinical claim
6.12 The submission claimed non-inferiority between voriconazole and posaconazole in terms of comparative effectiveness (incidence of proven or probable invasive fungal infection and all-cause mortality) and safety in high-risk patient populations (AML/MDS, GVHD, high-risk AlloHSCT).
6.13 The PBAC considered that despite the various factors that made the comparison of the clinical trials difficult to interpret, the submission’s clinical claim was likely to be reasonable.
Economic analysis
The submission presented a cost-minimisation analysis. The analysis included the main comparator, posaconazole, and the secondary comparators, fluconazole and itraconazole.
The equi-effective doses were estimated as voriconazole 200 mg twice a day is equal to:
- posaconazole 200 mg three times a day;
- fluconazole 400 mg once daily; and
- itraconazole 200 mg twice a day.
The equi-effective doses were appropriately derived from the dosage regimens used in the Wingard 2010, Ullmann 2007, Cornely 2007 and A1501073 trials.
6.14 The submission proposed a price for voriconazole used in prophylaxis. This price was used in the calculation of a weighted price for PBS listing based on the prices for treatment and prophylaxis indications. The results of a clinician survey commissioned by the sponsor were used as the basis of the estimation of the proportion of patients receiving prophylaxis compared to treatment with antifungal drugs.
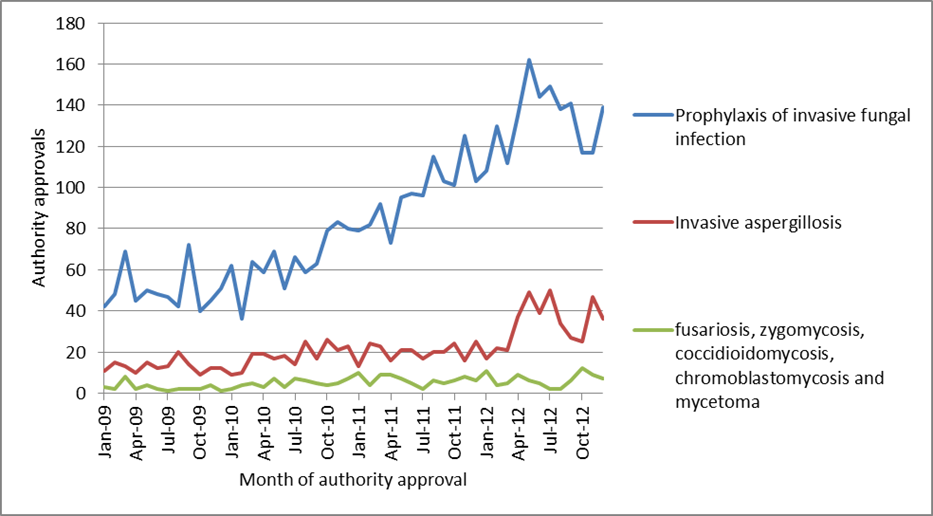
6.15 The PBAC considered that the clinician survey may not reliably reflect Australian practice given its low response rate (3.4%), high variation in answers of clinicians who did respond, the inclusions of respondents with reduced involvement in decision making regarding prophylaxis (e.g. infectious disease registrars) and missing data. The PBAC further noted the recent analysis (October 2013) provided by the Department showing the majority of Authority approvals for posaconazole were for prophylaxis. Additional analysis provided to the PBAC by the Department showed that in 2012, 76.6% of approvals for posaconazole were for prophylaxis.
6.16 The following figure shown below from the Department’s analysis show the authority approvals for posaconazole to December 2012 by indication.
Authority approvals for posaconazole to December 2012 by indication
Source: DHS-Medicare Authority Approval database, extracted July 2013
6.17 The submission’s proposed prophylaxis price based on average proportional utilisation sourced from the clinician survey is shown below:
|
Anti-fungala |
EED |
DPMQ |
Weightingb |
WDPMQ |
|---|---|---|---|---|
|
POSA |
200 mg tds |
|
(REDACTED) |
(REDACTED) |
|
ITRA |
200 mg bd |
(REDACTED) |
(REDACTED) |
(REDACTED) |
|
FLUC |
400 mg d |
(REDACTED) |
(REDACTED) |
(REDACTED) |
|
VORI |
200 mg bd |
|
(REDACTED) |
|
6.18 The PBAC noted that the evaluation had recalculated the price with different weightings (posaconazole, itraconazole, fluconazole weighting of (REDACTED)%, (REDACTED)% and (REDACTED)% respectively) resulting in a revised WDPMQ price of voriconazole of (REDACTED) (based on a voriconazole dose of 200 mg bd). The pre-sub-committee response did not agree with the alternative weighting calculated in the evaluation, arguing that there is currently some use of voriconazole as prophylaxsis (albeit not PBS subsidised for this indication) and therefore the weighting should be based on current clinical practice.
6.19 Having determined a price for voriconazole in prophylaxis the submission calculated a weighted price across prophylaxis and treatment indications based on a (REDACTED)%: (REDACTED)% distribution respectively. The prices of the various voriconazole dose presentations are shown below.
|
VORI |
Form |
DPMQ |
PTP |
Ex-man |
|
50 mg |
56 TAB |
(REDACTED) |
(REDACTED) |
(REDACTED) |
|
200 mg |
56 TAB |
(REDACTED) |
(REDACTED) |
(REDACTED) |
|
40 mg/ml |
1 POS (70 mL) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
6.20 The PBAC accepted the argument that because the usage of voriconazole as treatment was wider than posaconazole the uptake of voriconazole may not reflect the treatment vs. prophylaxis ratio as stated in the pre-PBAC response.
6.21 In summary, the PBAC considered that a cost-minimisation analysis against a weighted mixed comparator of posaconazole, fluconazole and itraconazole in the GVHD and AlloHSCT high risk patient populations to be appropriate. In these two patient groups (GVHD and AlloHSCT), the equi-effective doses were considered to be: voriconazole (200 mg twice daily); posaconazole (200 mg three times daily); fluconazole (400 mg daily) and itraconazole (200 mg twice daily). The weightings of posaconazole, fluconazole and itraconazole in the prophylactic setting should be: (REDACTED)%, (REDACTED)%, and (REDACTED)%.
6.22 In the AML/MDS high risk patient population, the PBAC considered a cost-minimisation comparison of voriconazole to fluconazole and itraconazole (not posaconazole) to be appropriate, based on the clinical evidence presented in the submission. The equi-effective doses were considered to be voriconazole 200 mg twice a day, fluconazole 400 mg daily and itraconazole 200 mg twice daily.
Estimated PBS usage & financial implications
6.23 The submission was not considered by DUSC.
6.24 The submission’s estimated use and financial implications are summarised in the following table:
|
|
Year 1 |
Year 2 |
Year 3 |
Year 4 |
Year 5 |
|
Estimated extent of use |
|||||
|
High-risk AlloHSCT population (epidemiological approach) |
|||||
|
Number treated |
(REDACTED) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
|
Market share |
(REDACTED) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
|
Scripts |
(REDACTED) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
|
AML/MDS neutropenia and GVHD population (market share approach) |
|||||
|
Market share |
(REDACTED) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
|
Scripts |
(REDACTED) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
|
Total scripts |
(REDACTED) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
|
Estimated total net cost to PBS/RPBS |
(REDACTED) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
(REDACTED) |
6.25 The submission estimated the net cost to the PBS of less than $10 million in year 5.
6.26 PBAC agreed with the ESC that the market share of voriconazole could possibly be greater than the 30% proposed in the submission as voriconazole does not require administration with a fatty meal, can be used in younger children and may be an easier formulation to administer. The PBAC also noted that the clinician survey did not provide a reliable estimate of use of prophylaxis and that there was potential for use beyond the requested indications into lower risk patient groups. The PBAC considered there were a number of issues with the utilisation estimates in the submission, including:
- Underestimation of the market share for voriconazole in the existing population, but this will take market from posaconazole for GVHD patients.
- Overestimation of the number of true high risk AlloHSCT patients. It is possible that a proportion of the medium risk AlloHSCT population will access treatment and this is use beyond the restriction.
- There is scope for growth of the overall market of eligible patients as posaconazole may be more difficult to use and there are advantages for voriconazole. This is likely to be small and may represent cost shifting from hospital budgets to Commonwealth budgets.
- The listing of voriconazole will replace some use of the less expensive fluconazole and itraconazole in the AlloHSCT and GVHD patient groups.
6.27 The PBAC noted the submission’s acceptance that the existing risk sharing arrangement will need to be amended. No details of an amended risk sharing arrangement were provided were provided in the submission. '(REDACTED)
6.28 (REDACTED)
7 PBAC Outcome
7.1 The PBAC recommended an extension to the listing of voriconazole to include an Authority required listing for prophylaxis against invasive fungal infections in the high risk patients groups of acute myeloid leukaemia (AML); high-risk myelodysplastic syndrome (MDS); Graft versus host disease (GVHD); and high risk allogeneic haematopoietic stem cell transplant (AlloHSCT) recipients.
7.2 The PBAC’s recommendation was on a cost minimisation basis against a weighted mixed comparator of posaconazole, fluconazole and itraconazole in the GVHD and AlloHSCT high risk patient populations. In these two patient groups (GVHD and AlloHSCT), the equi-effective doses are as follows: voriconazole (200 mg twice daily); posaconazole (200 mg three times daily); fluconazole (400 mg daily) and itraconazole (200 mg twice daily). The weightings of posaconazole, fluconazole and intraconazole in the prophylactic setting are: (REDACTED)%, (REDACTED)%, and (REDACTED)%.
7.3 In the AML/MDS high risk patient population, the PBAC recommended listing voriconazole on a cost-minimisation basis compared to only fluconazole and itraconazole. The equi-effective doses are voriconazole 200 mg twice a day, fluconazole 400 mg daily and itraconazole 200 mg twice daily.
7.4 The PBAC considered the submission’s proposed clinical place for voriconazole as an alternative antimicrobial for prophylaxis against invasive fungal infections, including both yeasts and moulds, to be reasonable.
7.5 The PBAC accepted posaconazole as the appropriate comparator. Fluconazole and itraconazole were also accepted by the PBAC as secondary comparators.
7.6 The PBAC noted that several of the studies presented in the submission had various confounding factors and biases, making it difficult for the PBAC to draw definitive conclusions on comparative effectiveness and safety, and, on the submission’s clinical claim. However, on balance, the PBAC considered that the evidence was suggestive of voriconazole being non-inferior in terms of efficacy to posaconazole for the AlloHSCT and GVHD patients groups, noting that the data was not entirely conclusive. The PBAC further considered that the clinical trial data in the AML/MDS high risk patient populations was inadequate in establishing non-inferiority between voriconazole to posaconazole. Instead, the PBAC considered that the evidence suggested that voriconazole is equivalent to fluconazole in this high risk patient population.
7.7 The PBAC accepted the overall cost minimisation approach in the economic analysis for the high risk patient populations of GVHD and AlloHSCT but not for the AML/MDS patient population. The PBAC considered the clinical trial data used to support listing in this patient population was inadequate in establishing non-inferiority between voriconazole and posaconazole. The PBAC was prepared to accept non-inferiority between voriconazole to fluconazole in AML/MDS high risk patients and so considered a cost-minimisation analysis in these circumstances to be more appropriate.
7.8 The PBAC considered there were various issues with the utilisation estimates in the submission and therefore recommended a risk sharing agreement between the sponsor and Commonwealth be entered into to limit utilisation in low risk patient populations and for indications other than prophylaxis.
7.9 The PBAC requested that the DUSC review use of voriconazole for the extended listing 12 months after the new listing is implemented.
Outcome
Recommended
Recommended listing
Add new indication:
|
Name, Restriction, Manner of administration and form |
Max qty (packs) |
Max. Rpts |
Proprietary Name |
Manufacturer |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
voriconazole Tablet, 50 mg, 56 |
1 | 0 | Vfend | PF | |||||||
|
Tablet, 200 mg, 56
Powder for suspension, 40 mg/mL, 70 mL, 1 |
1
1 |
0
0 |
Vfend
Vfend
|
PF
PF
|
|||||||
|
Indication: |
Prophylaxis of invasive fungal infections including both yeasts and moulds |
|||||||||
|
Restriction: |
Authority Required |
|||||||||
|
Clinical criteria:
|
Patient must be considered at high risk of developing an invasive fungal infection due to anticipated neutropenia (an absolute neutrophil count less than 500 cells per cubic millimetre) for at least 10 days whilst receiving chemotherapy for acute myeloid leukaemia or myelodysplastic syndrome
OR
Patient must be considered at high risk of developing an invasive fungal infection due to having acute graft versus host disease (GVHD) grade II, III or IV, or, extensive chronic GVHD, whilst receiving intensive immunosuppressive therapy after allogeneic haematopoietic stem cell transplant
OR
Patient must be undergoing allogeneic haematopoietic stem cell transplant using either bone marrow from an unrelated donor or umbilical cord blood (related or unrelated), and, be considered to be at high risk of developing an invasive fungal infection during the neutropenic phase prior to engraftment
|
|||||||||
|
Administrative Advice |
NOTE: For patients with graft versus host disease, acute myeloid leukaemia or myelodysplastic syndrome, applications for an increased maximum quantity to allow for up to 1 month’s treatment and repeats sufficient for up to 6 months’ treatment may be authorised.
For patients undergoing allogeneic haematopoietic stem cell transplant, applications for an increased maximum quantity to allow for up to 1 month’s treatment and repeats sufficient for up to 2 months’ treatment may be authorised.
Shared Cared Model: For prescribing by nurse practitioners where care of a patient is shared between a nurse practitioner and medical practitioner in a formalised arrangement with an agreed management plan. Further information can be found in the Explanatory Notes for Nurse Practitioners. |
|||||||||
Context for Decision
The PBAC helps decide whether and, if so, how medicines should be subsidised in Australia. It considers submissions in this context. A PBAC decision not to recommend listing or not to recommend changing a listing does not represent a final PBAC view about the merits of the medicine. A company can resubmit to the PBAC or seek independent review of the PBAC decision.
Sponsor’s Comment
Pfizer Australia (the Sponsor) welcomes the PBAC recommendation to list voriconazole for prophylaxis against fungal infections in patients at high risk of developing these infections.

