
Submission to Post-Market Review of PBS Medicines Used to Treat Asthma in Children
Submission 9 - GlaxoSmithKline
Thank you for your letter dated 7 February 2013 requesting input into the proposed review of Pharmaceutical Benefits Scheme (PBS) medicines used to treat asthma in children. This response will concentrate on addressing items 3 to 5 of the Terms of Reference of the review.
GlaxoSmithKline provided a summary of the clinical evidence for the use of its fixed dose combination (FDC) product, Seretide® (fluticasone propionate with salmeterol xinafoate) in children in previous correspondence relating to the Drug Utilisation Sub-Committee (DUSC) report on utilisation of combination inhaled corticosteroid (ICS) and long acting beta agonist (LABA) dated 26 August 2011.
GSK considers the appropriate use of its medicines to be a core principle, and undertakes to ensure products are promoted and used in line with the highest ethical, medical and scientific standards. In line with this, and despite a Therapeutic Goods Administration (TGA) registered indication that permits utilisation from 4 years of age, GSK has never conducted promotional activities for the company's FDC product, Seretide (fluticasone propionate with salmeterol xinafoate) in relation to use within this specific age group. GSK representatives do not discuss Seretide's paediatric indication or usage, and there has been no advertising relating to use in any paediatric population.
GSK have proactively sought to address potential inappropriate use of ICS/LABA in recent years through a number of activities aimed at improving the quality use of medicine in paediatric asthma. Additionally, GSK Australia has engaged with expert paediatricians in order to understand possible explanations of this usage pattern, and to consider what action could practicably be undertaken to reduce inappropriate usage of ICS/LABA in children.
GSK has consulted general practitioners (GPs) and specialist respiratory clinicians to assist with informing GSK’s response to the Terms of Reference (items 3-5).
Terms of Reference – Item 3.
Identify areas of prescribing for childhood asthma in Australia where clinical practice is inconsistent with clinical guidelines; and if there is evidence that supports this practice.
Discussions with clinicians regarding current treatment of childhood asthma are generally reflective of the DUSC review findings suggesting the treatment of childhood asthma not currently aligned with the Australian and Global guidelines of a step up treatment regime beginning with short acting beta agonist (SABA), then monotherapy ICS then if necessary step up to a FDC.
There are several reasons given why current practice may not be aligned with the guidelines provided by the clinicians:
- Parents’ desire for quick relief of their child’s asthma and provision of a FDC is an easy solution that will keep the child and parent ‘happy’; if the parent was not satisfied with the level of relief they would seek treatment from another GP, this was referred to as ‘GP Shopping’.
- It has been expressed that diagnosis of asthma may improve as children age as the patient history becomes clearer. It is felt that there may be some misdiagnosis of viral associated wheeze as asthma among GPs. This is consistent with recent analyses of the Longitudinal Study of Asthma in Children (LSAC) data that indicate that by the age of 4–5 years, nearly a quarter (24.4%) of children had reported asthma or wheeze at some stage. However, not all wheeze qualifies as asthma and by age 4–5 years the incidence of wheeze, at 21.7%, was nearly double that of diagnosed asthma (11.5%). In contrast, among children aged 8–9 years, the incidence of asthma (16.3%) and wheeze (15.2%) over the past 4 years were similar. However, the DUSC report does not confirm that the children receiving a single ICS/LABA script do not have asthma or have subsequently no asthma symptoms. Poor asthma control (frequent symptoms and asthma exacerbations) remains a common problem in children (Asthma in Australia 2011). These data could indicate intermittent use of ICS/LABA by children with asthma and potentially reflect poor adherence to medical advice.
- There is no clear differentiation in the treatment of adult and children; there is a clear distinction in approach to treatment for children under 5, however the differentiation between adult treatment and child treatment is not clear enough for ages 8-14.
- Inappropriate prescribing from tertiary institutions influencing GP prescribing has been described with children discharged on FDC inhalers and high dose oral corticosteroids with parents subsequently expecting the same treatment from their GP.
However, analysis of the DUSC report is difficult as it is usually not possible to determine from survey data or prescription data whether the level of treatment that was prescribed or dispensed is appropriate for the patient’s level of disease severity or control (Khan et al. 2003). In the absence of information on disease severity and control, information on the use of medications must be interpreted with caution (Asthma in Australia 2011).
Terms of Reference – Item 4.
Identify and review recent (past five years) healthcare professional and consumer education in the area of medication management in children with asthma.
Clinicians report that most of the healthcare professional education that has been conducted has been focused on adult asthma and not childhood asthma. A pharmaceutical sponsor had provided specific education on childhood asthma in the past, but not recently.
GSK suggests that an independent and comprehensive program could be developed and shared with multiple organisations such as the National Prescribing Service (NPS), Medical Local divisions, and patient organisations, for use in their educational activities. It is preferred that these bodies are responsible for delivery of the education as they are well respected, independent and have a wide reach. There is also a need for user friendly educational activities such as Webinars with continuing professional development (CPD) points attached to further learning and development.
Paediatric Respiratory Taskforce
ln August 2009, GSK convened a panel of five expert paediatricians and a GP with a view to obtaining consensus on how best to achieve quality use of Seretide in paediatric patients. The agenda included identifying key concerns and consideration of appropriate educational messages, and appropriate forums to address them. Key concerns identified, predominately in primary care, included:
- Combination ICS/LABA therapy was being used first line without prior ICS monotherapy.
- Combination ICS/LABA therapy was being used in mild, episodic asthma, and for exacerbation management.
- Combination ICS/LABA therapy was being used to control symptoms, (e.g. coughing, wheezing) without prior diagnosis of asthma.
- Combination ICS/LABA therapy being used in patients under 4 years old.
The consensus reached was that in order to ensure the quality use of Seretide:
- Steps needed to be taken to ensure that ICS monotherapy is used first line, in accordance with guidelines.
- Steps needed to be taken to ensure that a correct diagnosis is made, especially in preschoolers and children with cough only.
The panel considered a number of potential initiatives that could be undertaken to implement the above education. A short list of four initiatives was identified and is outlined below. To date all have been successfully implemented, either by the panel alone, or as a collaborative effort with GSK.
1. Publication of The Role of Corticosteroids in the Management of Childhood Asthma. The Thoracic Society of Australia and New Zealand. Official position statement, 2017.
This paper was published just prior to the annual Thoracic Society of Australia and New Zealand (TSANZ) conference in March 2011, allowing for comment and review at this meeting. The paper was additionally reviewed by the paediatric special interest group for comments. lt represents endorsement from the region's leading professional society and gives a platform to reinforce the appropriate management of paediatric asthma. lt is of relevance to both specialists and GPs.
This article reinforces the evidence base for:
- Role of non-steroid preventers (e.g. Leukotriene Receptor Antagonists (LTRAs) - montelukast) in frequent intermittent or mild persistent asthma, and in patients with exercise induced symptoms.
- Role of ICS monotherapy as a first line preventer treatment in moderate to severe persistent asthma, or as an alternative to non-steroid preventers in frequent intermittent or mild persistent asthma.
- The appropriate initial daily dose of ICS (400 mcg beclomethasone (BDP) or equivalent).
- The appropriate role of LABA only as a step up addition for children aged five or older who are uncontrolled on an ICS dose of 400mcg BDP or equivalent.
- Selection of an age appropriate device and tuition of inhaler technique.
- Steps to take to reduce oro-pharyngeal deposition (spacers, mouth rinsing).
- Specialist referral of children requiring high doses of lCS.
2. Educational Tool- "Drive Time" Audio CD June 2011
GSK Australia sponsored the creation and distribution of a session on the popular "Drive Time" audio CD series for GPs. The 'Drivetime Medical' programme is a regular audio CD series that is distributed on a complimentary basis to over 21,000 GPs throughout Australia. All programmes are also available for listening on-line or to download. The program focused on the management of paediatric asthma and the appropriate use of the different medications. On the CD specialist Professor Nick Freezer was interviewed and during the discussion he reinforced the importance of the role of initial preventers such as ICS monotherapy / montelukast, and the appropriate addition of LABA and use of FDC ICS/LABA, such as Seretide. Prof Freezer also discussed the fact that the majority of children do not need a preventer and can be managed on SABA alone.
3. National CME accredited - Experts on air weekend educational meeting series
ln 2011 GSK sponsored a national educational meeting series with a focus on respiratory management. The content was prepared by an independent medical education agency. The series included a specific session on Paediatric asthma diagnosis and management, and outlined guideline management of paediatric asthma. The series involved 9 meetings nationally.
4. Sponsorship of a debate on the appropriate management of paediatric asthma at the National GP congress - General Practitioner Conference and Exhibition (GPCE), Sydney 2010
GSK sponsored a plenary session which involved a debate on the appropriate management of paediatric asthma. The chair of the Paediatric Respiratory Taskforce (Dr. Craig Mellis) chaired this session and spoke as one of the debaters. There was a lively discussion, a long Q&A session, and during the meeting, the appropriate use of ICS monotherapy, and the appropriate use of ICS/LABA was discussed and reinforced.
Terms of Reference – Item 5.
Identify effective interventions that have resulted in improvement of prescribing and quality use of medicines in the context of childhood asthma using overseas or Australian literature.
GSK conducted a literature search and identified a number of publications relating to programs designed to improve the treatment of paediatric asthma. These are summarised in Table 1.
Table 1: Publications of studies designed to improved paediatric asthma treatment
|
Author |
Title |
Publication |
|---|---|---|
|
Baldacci S, Maio S, Simoni M et al |
The ARGA study with general practitioners: impact of medical education on asthma/rhinitis management. |
Respiratory Medicine 2012; 106: 777-85. |
|
Braido F, Comaschi M, Valle I et al |
Knowledge and health care resource allocation: CME/CPD course guidelines-based efficacy |
Eur Ann Allergy Clin Immunol 2012: 44(5): 193-99. |
|
Davis AM, Cannon M, Ables AZ, Bendyk H |
Using the electronic medical record to improve asthma severity documentation and treatment among family medicine residents |
Family Medicine 2010; 42(5): 334-7. |
|
Liaw S-T, Sulaiman ND, Barton CA et al |
An interactive workshop plus locally adapted guidelines can improve General Practitioners asthma management and knowledge: a cluster randomised trial in the Australian setting |
BMC Family Practice 2008; 9: 22-9. |
|
Shah S, Sawyer SM, Toelle BG |
Improving paediatric asthma outcomes in primary health care: a randomised controlled trial. |
MJA 2001: 195(7): 405-9. |
|
Shapiro A, Gracy D, Quinones W et al |
Putting guidelines into practice. Improving documentation of pediatric asthma management using a decision-making tool. |
Arch Pediatr Adolesc Med 2011; 65(5): 412-8. |
|
Urrusuno RF, de la Pisa BP, Balosa MCM |
Impact of postal prescriber feedback on prescribing practice of Andalucian primary care paediatricians. |
Journal of Pharmaceutical Health Services Research 2011: 2: 113-20. |
These studies show an improvement in asthma diagnosis, treatment or patient education following the implementation of a medical education program. One study, conducted in Australia, showed an improvement in the prescribing of inhaled corticosteroids and long-acting beta agonists in children (Shah et al, 2011).
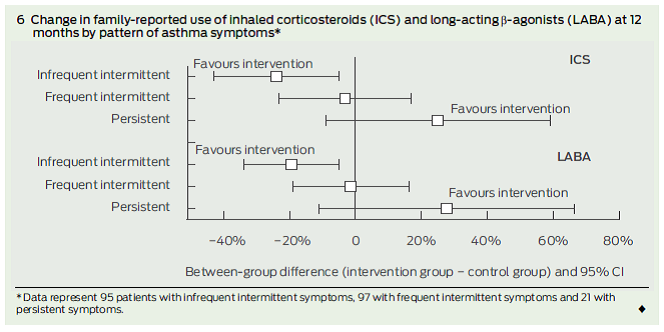
Shah et al (2011) conducted a study designed to evaluate the effectiveness of the Practitioner Asthma Communication and Education (PACE) Australia program. The study was conducted in General Practices from two regions in Sydney and recruited 150 GPs between 2006 and 2008. GPs were split into 2 groups with one group (the intervention group) participating in two 3-hour workshops, focusing on communication and education strategies to facilitate quality asthma care. The study determined that the intervention group prescribed children with infrequent, intermittent asthma symptoms significantly lower amounts of ICS (-24%; 95% CI: -43% to -5%) and LABA (-19%; 95% CI: -34% to -5%) as indicated in Figure 1. The study concluded the PACE Australia program improved GPs’ asthma management practices.
Figure 1: Change in ICS and LABA use by pattern of asthma symptoms (Shah et al, 2011)
Conclusion
When used appropriately, Seretide has a legitimate role in asthma management of paediatric populations. Evidence demonstrating the impact of treatment, specifically in these young patients, supports the TGA registration, PBS listing and guideline support of its use in children over 4 years of age.
GSK has been proactive in reinforcing the appropriate use of medicine in the management of paediatric asthma. As a result, and although Seretide has a licensed indication for the treatment of asthma in children aged four and above, GSK has never conducted promotional activities or advertising concerning this indication within this specific age group.
GSK supports the development of a paediatric asthma specific medical education program delivered by multiple respected groups. There is Australia specific evidence supporting the positive impact of medical education on appropriate prescribing of ICS and LABA in children. This supports the development of paediatric asthma specific professional education program(s) to be run by independent and respected parties such as the NPS, Medicare Locals and patient organisations which will improve appropriate prescribing of all asthma medications in children.
In developing this response, GSK has considered all options available that may impact the prescribing of FDC’s to children. GSK considers that the current PBS restriction level for prescribing of FDCs is appropriate and any change to this is beyond the Terms of Reference of the review. There are no clinical data supporting an improvement in the management of paediatric asthma as a consequence of more rigorous reimbursement criteria.
Further, GSK has significant concerns that application of more rigorous reimbursement criteria of FDC’s to children may be impractical and have adverse clinical consequences. Age specific PBS restrictions would be inconsistent with registered indications for these if applied across all FDCs and all strengths. Imposing greater restriction solely to the reimbursement criteria of FDCs registered for paediatric use (the lowest dose of Seretide) may inadvertently result in the increased prescribing of higher dose FDC’s or other FDC’s unregistered for paediatric use.
Kind regards,
Riona Hanley
Manager, Reimbursement and Pricing
GlaxoSmithKline Australia

